How Foot and Ankle Surgeons Can Benefit From PRP

Since it is a new science, many people are skeptical about Platelet-Rich Plasma, otherwise known as PRP. There are some studies out there that state that PRP work no better than a similarly administered placebo, but there are many other studies and doctors that claim that PRP works and works well. This also works well at a much lower cost and less side effects, than traditional medicine.
One branch where the skepticism is loud and clear is podiatry, which deals with feet and ankles. Trying to combat this skepticism can help many surgeons to lower complication rates, improve patient satisfaction, and have better outcomes. For instance, here is a list of cases where PRP has been effective for the feet and ankles.
- Plantar Fasciitis
PRP has become rather common as a treatment for Plantar Fasciitis, with many studies to prove the efficacy of this treatment. For instance, Dr. Daanial Kassicieh or Sarasota Neurology claims that PRP is one of the most effective treatments for this condition, and that PRP is actually fully cure it. Many of his patients have avoided surgery just by utilizing PRP therapy.
This is done with no down time, no rehabilitation, and no side effects. This woud explain why plantar fasciitis is the 5th popular medical condition treated by PRP. This can be explained by over 3 million people that are diagnosed with this and no other treatment really works for it, besides, in fact, PRP.
- Archilles Tendonitis
This is another condition that can be fairly hard to treat, and gets worse over time unless healed. Many surgical approaches are often trickey and generally do not end up with good results. Because of this, the main treatment option is simply to give patients corticosteroids to reduce the pain, but really nothing else to treat the symptoms.
However, there have been many studies done that have shown that PRP is a lot more effective, including that from the European Foot and Ankle Society. This means that PRP is safer and more effective alternative than any other treatments available.
- Diabetic Foot Ulcers
Diabetic foot ulcers can be troublesome, especially when they do not heal or heal properly. Over 2.5 million Americans with diabetes who suffer from these ulcers. About 11% of these cases may need amputation of their affected limb. However, some studies have noted that just one injection of PRP and a topical solution bi-weekly started to heal the ulcers in just 8 weeks. Topical PRP also has been shown to work better than anti-septic creams as well.
- Regenerating Bones
Bone regeneration is most commonly needed in food and ankle area. Although mechanical stabilization works best, the utilization of PRP has been surprising. PRP helps with healing bones and soft tissue at the damage site. According to a recent systematic review of 64 articles, the conclusion was to include more PRP therapy into the healing of foot and ankle bones.
The science behind this is solid, for bone or tissue to form, three things are needed in the area:
- A scaffold for the growth to take place
- Biological stimulants to signal proteins
- Stem cells that provide bone building potential
All three of these are crucial for bone formation.. PRP can provide at least two of these, so there is no reason to ignore it when it comes to bone regeneration.
- Ankle Sprains
This is an incredibly common condition, and can be effectively treated by using PRP therapy. In one randomized controlled trial, researchers studied the effects of PRP injections on athletes with ankle sprains. This study showed that not only did PRP reduce the healing time by 20 days, but that they also experienced much less pain. This can reduce the recovery period from 6 weeks, for just about 2 or 3 weeks.
Immobilization is Vital
When it comes to foot and ankle related injuries, one thing that really cannot be avoided in rest and rehabilitation. This is true regardless of whether PRP is administered. Because of this, many of the studies that shows PRP to be ineffective often don’t use rest and rehabilitation, and that alone can be an issue.
PRP is in no way a magic pill. All foot injuries need rest and rehabilitation in order to properly heal. With these two combined, it can drastically reduce healing times.
How can Foot and Ankle Surgeons Benefit?
Using PRP in foot and ankle injuries is not going anywhere, so utilizing it would be the best way to go. Test it out with your patients, and try using platelet-rich plasma therapy instead of simply prescribing pills or doing costly surgeries. Your patients will thank you in the end.

- Published in Blog
Stem Cell Research Goes Crimson: International Leader in Stem Cell Research Named New Dean of Harvard Medical School

George Q. Daley, MD, PhD, Harvard Medical School’s newly appointed dean, led dozens of international colleagues in developing ethical guidelines for stem cell research. On March 9, 2009, President Barack H. Obama issued Executive Order 13505: Removing Barriers to Responsible Scientific Research involving Human Stem Cells, stating that the Secretary of Health and Human Services, through the Director of the National Institute of Health (NIH), may support and conduct responsible, scientifically worthy human stem cell research, including human embryonic stem cell (hESC) research, to the extent permitted by law. Internal NIH policies and procedures, consistent with Executive Order 13505 and these Guidelines, govern the conduct of intramural NIH stem cell research.
A prominent stem cell researcher has been named the new dean of Harvard Medical School, the university announced August 9th
George Q. Daley, MD, PhD, who led dozens of international colleagues to unite around ethical guidelines for stem cell research, is taking on a new challenge—unifying the powerful hospitals that train Harvard’s medical students.
taking on a new challenge—unifying the powerful hospitals that train Harvard’s medical students.
Daley will assume the position effective Jan. 1, 2017, succeeding Jeffrey Flier, MD, who stepped down July 31st. Barbara McNeil, MD, the founding head of the Department of Health Care Policy at Harvard Medical School, is filling the position in the interim.
The internationally recognized leader in stem cell science and cancer biology and a longtime member of the Harvard Medical School (HMS) faculty whose work includes the fields of basic science and clinical medicine, Daley was the driving force behind creating international guidelines around first, human embryonic stem cell research, and then the clinical application of stem cells, according to Nancy Witty, CEO of the International Society for Stem Cell Research (ISSCR).
Daley, who cofounded the organization, counseled two dozen scientists through the sensitive ethical discussions involved in establishing stem cell research guidelines, utilized additional input from 60 groups around the world to construct the guidelines which were first published by the National Institute of Health in 2009.
“That’s a very difficult task,” Witty said. “It takes a tremendous amount of diplomacy.” 
Daley is working to adapt insights in stem cell research to improved therapies for genetic and malignant diseases. Important research contributions from his laboratory at Harvard-affiliated Boston Children’s Hospital include the development of customized stem cells to treat genetic immune deficiency in a mouse model (in collaboration with Rudolf Jaenisch, a Professor of Biology at MIT); the differentiation of germ cells from embryonic stem cells (cited as a “Top Ten Breakthrough” by Science magazine in 2003), and the generation of disease-specific pluripotent stem cells by direct reprogramming of human fibroblasts (cited in the “Breakthrough of the Year” issue of Science magazine in 2008).
As a graduate student working with Nobel laureate Dr. David Baltimore, Daley demonstrated that the BCR/ABL oncogene induces chronic myeloid leukemia (CML) in a mouse model, which validated BCR/ABL as a target for drug blockade and encouraged the development of imatinib (GleevecTM; Novartis), a revolutionary magic-bullet chemotherapy that induces remissions in virtually every CML patient. Dr. Daley’s recent studies have clarified mechanisms of Gleevec resistance and informed novel combination chemotherapeutic regimens.
Daley has spent his entire career in Cambridge and Boston, earning a medical degree from Harvard and a PhD in biology from MIT. As Dean of Harvard Med School, Daley’s achievements in stem cell research is expected to shine a distinguished light on the stem cell industry.
Although the position of dean of Harvard Med may be one of the most prominent roles in medicine, the position is not as powerful it might seem: Harvard Med does not directly oversee any hospitals. Instead it relies on 15 affiliated hospitals and clinical sites, which have historically operated as separate, competitive bailiwicks, to train its students and postdoctoral fellows, and support its researchers. Only 151 of the nearly 12,000 people who call themselves Harvard Medical faculty actually work directly for Harvard in its 10 basic science departments.
Daley sees his new position as a congregator who “builds bridges among the institutions” —heavyweight research institutions such as Brigham and Women’s, Massachusetts General, and Boston Children’s hospitals. Persuasiveness, rather than power, is all that Daley says is needed to achieve an alliance.
Daley’s predecessor, Flier, says he spent a full 30 percent to 40 percent of his time as dean trying to build relationships with and coordinate Harvard’s affiliated hospitals and clinics, a challenge Daley says he’s up to. He has a head start in building those relationships through the many positions he has held around Boston’s biomedical community, including chief resident at Mass. General
“My vision is one of increasing connectivity across the community,” Daley says.
Currently a professor of biological chemistry and molecular pharmacology at Harvard Medical School and director of the stem cell transplantation program at Boston Children’s and Dana-Farber Cancer Institute, Daley sees areas of common interest, such as immuno-oncology, which harnesses the body’s own immune system against cancer cells, where the hospitals can work more closely together.
Described by colleagues as a natural leader, Daley recently led an effort to coordinate big-name scientists across several institutions on a collaborative grant to compare two types of stem cells—just one example of how he earned a reputation; he knows how to get different groups talking together in a constructive way.
He also says he wants Harvard Medical’s faculty, students, and staff to reflect the global community the school intends to serve, and that he promotes diversity in hiring for his 30-person lab.
Daley has a keen interest in sickle-cell anemia, which affects people of African descent, including African Americans, and he believes the federal government should invest in a moonshot effort to cure the disease.
Daley plans to continue teaching molecular medicine at Harvard Med after assuming his position as dean. He also plans to spend one day per week in his lab researching blood stem cells.
“It’s important for a dean to remain relevant by continuing to publish papers,” Daley says. “Plus, I just love science.”
Among his priorities is raising money. Despite its worldwide reputation, and its relative influence when it comes to landing federal grants, Harvard Med has seen annual deficits of between $31 million and $45 million for three consecutive years. Suggestions are being made for Harvard to rename its medical school in return for a billion-dollar donation. Daley only says that the idea would be worth considering down the road.
With opportunities for federal grants in decline, Daley says he sees an opportunity to bring in money from corporate partnerships.
For the stem cell research and medical community, Daley’s appointment as dean of Harvard Med is a fitting step toward validating regenerative medicine’s place as an authoritative leader in the future of medicine—one that’s been a long time coming.
Learn more about Dr. Daley here.
###

- Published in Blog
Insulin-producing Stem Cells Grown in the Lab Mark a New Era in Stem Cell Therapies for Diabetes

A new discovery by researchers on how to activate lab-grown beta cells to mature into functioning cells that produce and release insulin in response to glucose take a significant step toward a cell therapy treatment for diabetes.
Difficulties in manipulating beta cells derived from human stem cells to mature beyond the precursor stage into fully functioning insulin releasers has been an on-going challenge for researchers..
However, researchers from the Salk Institute for Biological Studies and a team of researchers have achieved this goal with lab-grown beta cells by activating a protein called estrogen-related receptor γ (ERRγ). Their study findings were recently published in the journal Cell Metabolism.
Self-renewing capacity of human pluripotent stem cells (hPSCs)
Ronald Evans, senior author of the study, titled, “ERRγ Is required for the Metabolic Maturation of Therapeutically Functional Glucose-Responsive β Cells,”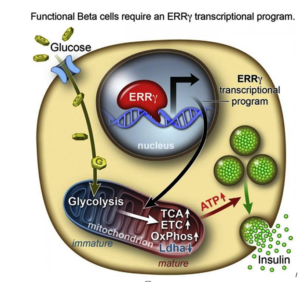 says the self-renewing capacity of human pluripotent stem cells (hPSCs) and their ability to differentiate into most cell types—from neurons to skin cells, to muscles cells and insulin-producing pancreatic beta cells—has inspired many research teams to find ways to make glucose-responsive beta cells in the lab.
says the self-renewing capacity of human pluripotent stem cells (hPSCs) and their ability to differentiate into most cell types—from neurons to skin cells, to muscles cells and insulin-producing pancreatic beta cells—has inspired many research teams to find ways to make glucose-responsive beta cells in the lab.
Evans and his research team discovered the answer to the insulin-releasing cell conundrum, and summed it up thusly:
“In a dish, with this one switch, it’s possible to produce a functional human beta cell that’s responding almost as well as the natural thing.”
Evans, a molecular biologist at the Salk Institute, says that to create the different types of cells in the lab, researchers coax the pluripotent stem cells (hPSCs) down the various branching paths that fetal cells normally travel in order to differentiate into the various cell types. However, he explains there are many developmental points in this process, and in the case of lab-grown pancreatic beta cells, research kept getting stuck at an early stage.
Adult beta cells have more ERRγ protein for a very energy-intensive process
In order to determine what might trigger the next step in getting the cells to mature, the researchers compared transcriptomes of adult and fetal beta cells. The transcriptome contains, among other things, the full catalog of molecules that switch genes on and off in the genome, which led them to discover that the nuclear receptor protein ERRγ was more abundant in adult beta cells. The team was already familiar with the protein’s role in muscle cells and had studied its ability to enhance endurance running.
Evans says that in muscles, protein promotes greater growth of mitochondria—the power generators inside cells that accelerate the burning of sugars and fats to make energy.
“It was a little bit of a surprise to see that beta cells produce a high level of this regulator,” Evans says. “But beta cells have to release massive amounts of insulin quickly to control sugar levels. It’s a very energy-intensive process.”
The research team then decided to run some tests to look more closely at what role ERRγ might play in insulin-producing beta cells.
A new era in creating functional, insulin-producing beta cells
 After they genetically engineering a deficiency of ERRy in mice, the researchers found the animals’ beta cells did not produce insulin in response to spikes in blood sugar.
After they genetically engineering a deficiency of ERRy in mice, the researchers found the animals’ beta cells did not produce insulin in response to spikes in blood sugar.
Next they tried to get beta cells made from hPSCs to produce more ERRγ, and it worked! The cells in culture began to respond to glucose and release insulin.
Finally, the team transplanted the lab-grown insulin-producing beta cells into diabetic mice and found that from day one, the cells produced insulin in response to glucose spikes in the animals’ blood.
Evans and the research team were justifiably excited by the results. It appears that just switching on the ERRγ protein is sufficient to get the lab-grown beta cells to mature and produce insulin in response to glucose – both in cultures and in live animals.
Speculating on the implications of their findings, Evans suggests that when a fetus is developing, because it gets a steady supply of glucose from the mother, it does not need to produce insulin to regulate its blood sugar, so the switch is inactive. But, when the baby is born and takes its first breath and takes in oxygen, this activates the switch.
Previous lab attempts to produce beta cells got stuck at the fetal stage. The Salk Institute researchers discovered how to take it to the adult stage, using the same protein that is switched on in nature.
“I believe this work transitions us to a new era in creating functional beta cells at will,” Evans says.
He and his research team now plan to examine how the switch might work in more complex models of diabetes treatments.
The Salk Institute study proceeds another study Medical News Today in which researchers generated mini-stomachs that produce insulin when transplanted into mice.
###
- Published in Blog
Regenerating and Restoring Brain Cells in the Aged With Donor Neural Stem Cells

The human brain, as it turns out, is far more malleable than we once thought. Even adult brains. But they are subject to age-related diseases and disorders, such as dementia and diminished cognitive function.
There is hope that medical science may be able to replace brain cells and restore memory in aging patients thanks to new discoveries in neural stem cell techniques. Researchers at the Texas A&M Health Science Center College of Medicine recently published new findings in the journal Stem Cells Translational Medicine that suggests a new technique for preparing donor neural stem cells and grafting them into an aged brain can regenerate tissue that has succumbed to structural, chemical, and functional changes, as well as a host of neurocognitive changes that can be attributed to aging.
The study, titled “Grafted Subventricular Zone Neural Stem Cells Display Robust Engraftment and Similar Differentiation Properties and Form New Neurogenic Niches in the Young and Aged Hippocampus,” was led by Ashok K. Shetty, Ph.D., a professor in the Department of Molecular and Cellular Medicine. associate director of the Institute for Regenerative Medicine, and research career scientist at the Central Texas Veterans Health Care System.
Shetty and his team at Texas A&M focus on the aged hippocampus, which plays an important role in making new memories and connecting them to emotions. They took healthy donor neural stem cells and implanted them into the hippocampus of an animal model, essentially enabling them to regenerate tissue.
The hippocampus in the aging brain
“We chose the hippocampu s because it’s so important in learning, memory and mood function,” Shetty said. “We’re interested in understanding aging in the brain, especially in the hippocampus, which seems particularly vulnerable to age-related changes.”
s because it’s so important in learning, memory and mood function,” Shetty said. “We’re interested in understanding aging in the brain, especially in the hippocampus, which seems particularly vulnerable to age-related changes.”
The volume of this part of the brain seems to decrease during the aging process, and this decrease may be related to age-related decline in neurogenesis (production of new neurons) and the memory deficits some people experience as they grow older.
The aged hippocampus also exhibits signs of age-related degenerative changes in the brain, such chronic low-grade inflammation and increased reactive oxygen species.
Bharathi Hattiangady, assistant professor at the Texas A&M College of Medicine and co-first author of the study said his team was excited to discover that the aged hippocampus can accept grafted neural stem cells as well as the young hippocampus does, a discovery that has significant implications for treating age-related neurodegenerative disorders.
“It’s interesting that even neural stem cell niches can be formed in the aged hippocampus,” Hattiangady says.
 Shetty’s previous research focused on the benefits of resveratrol (an antioxidant that is famously found in red wine and the skin of red grapes, as well as in peanuts and some berries) to the hippocampus. Although the results indicated important benefits for preventing memory loss in aging brains, his newest work demonstrates a way to affect the function of the hippocampus more directly.
Shetty’s previous research focused on the benefits of resveratrol (an antioxidant that is famously found in red wine and the skin of red grapes, as well as in peanuts and some berries) to the hippocampus. Although the results indicated important benefits for preventing memory loss in aging brains, his newest work demonstrates a way to affect the function of the hippocampus more directly.
Neural stem cell grafting
In this new study, the team found that the neural stem cells engrafted well onto the hippocampus in the young animal models (which was expected) as well as the older ones that would be, in human terms, about 70 years old. Not only did these implanted cells survive, they divided several times to make new cells.
“They had at least three divisions after transplantation,” Shetty said. “So the total yield of graft-derived neurons and glia (a type of brain cell that supports neurons) were much higher than the number of implanted cells, and we found that in both the young and aged hippocampus, without much difference between the two.”
 In both old and young brains, a small percentage of the grafted cells retained their stemness feature—an essential characteristic of a stem cell that distinguishes it from ordinary cells—and continuously produced new neurons. This is called creating a new ‘niche’ of neural stem cells, and these niches seemed to be functioning well. They were still producing new neurons at least three months after implantation, and these neurons are capable of migrating to different parts of the brain.
In both old and young brains, a small percentage of the grafted cells retained their stemness feature—an essential characteristic of a stem cell that distinguishes it from ordinary cells—and continuously produced new neurons. This is called creating a new ‘niche’ of neural stem cells, and these niches seemed to be functioning well. They were still producing new neurons at least three months after implantation, and these neurons are capable of migrating to different parts of the brain.
Past efforts to rejuvenate brains using fetal neurons in this way weren’t nearly as successful. Immature cells, such as neural stem cells, seem to do a better job because they can tolerate the hypoxia (lack of oxygen) and trauma of the brain grafting procedure better than post-mitotic or relatively mature neurons. When researchers tried in the past to implant these partially differentiated cells into the aged hippocampus, they didn’t do nearly as well. The research team used a new technique of preparing the donor neural stem cells, which Shetty says is why this result has never been seen before.
Brain marrow
The researchers used donor cells from the sub-ventricular zone of the brain, an area called the “brain marrow,” because it is analogous to bone marrow in that it holds a number of neural stem cells that persist throughout life. These neural stem cells continuously produce new neurons that migrate to the olfactory system. They also respond to injury signals in conditions such as stroke and traumatic brain injury and replace some of the lost cerebral cortical neurons.
Induced pluripotent cells from skin
Even a small stem cell sample is good enough to expand in culture, so the procedure isn’t terribly invasive. However, in the future, a single skin cell might suffice, as similar neural stem cells can be obtained in large numbers from skin. In fact, it is well known in medical science that a number of cells in the body—including skin cells—can be modified in such a way to create induced pluripotent stem cells.
With these cells, scientists can do any number of things, such as making neural stem cells that will make both more of themselves, and make new neurons. It’s not necessary to get the cells from the brain, just take a skin biopsy and push them into neural stem cells, according to Shetty.
Although the way the grafted cells thrived is promising, there is still a good deal of work to be done to determine if the extra grey matter actually improves cognition.
“Next, we want to test what impact, if any, the implanted cells have on behavior and determine if implanting neural stem cells can actually reverse age-related learning and memory deficits,” Shetty said. “That’s an area that we’d like to study in the future.
“I’m always interested in ways to rejuvenate the aged brain to promote successful aging, which we see when elderly persons exhibit normal cognitive function and the ability to make memories.”
###
- Published in Blog
Stem Cell-stimulating Fillings Help Regenerate Teeth Damaged by Disease, Decay

Researchers from Harvard University and the University of Nottingham have developed a new filling that stimulates stem cells in dental pulp to regenerate and even regrow teeth damaged by disease and decay. According to Newsweek Magazine, the discovery earned a prize from the Royal Society of Chemistry after judges described it as a “new paradigm for dental treatments.”
The treatment is believed to potentially eliminate the need for root canals.
Filling materials stimulate stem cells to encourage dentin growth
The filling works by stimulating the body’s natural store of stem cells to encourage the growth of dentin—the bony material that makes up the majority of the tooth—allowing patients to effectively regrow teeth that are damaged through dental disease. The filling’s synthetic biomaterials are used similarly to dental fillings, placed in direct contact with pulp tissue in the damaged tooth. This stimulates the tissue’s native stem cell population to repair and regenerate pulp tissue and the surrounding dentin.
The discovery is a significant step forward from current methods to treat cavities, which involve drilling out decay and putting in a filling made of gold; porcelain; silver amalgam (which consists of mercury mixed with silver, tin, zinc, and copper); or tooth-colored plastic or composite resin. When these fillings fail to halt the tooth’s decay, a root canal is needed to remove the pulp of the tooth, damaging it even further.
Alternative to traditional fillings in teeth
Researchers hope to develop the technique with industry partners in order to make it available for dental patients as an alternative to traditional fillings. Marie Curie research fellow Adam Celiz says that existing dental fillings are toxic to cells and are therefore incompatible with pulp tissue inside the tooth.
“In cases of dental pulp disease and injury, a root canal is typically performed to remove the infected tissues,” Celiz says.
The promise of using therapeutic biomaterials to bring stem cell medicine to restorative dentistry could significantly impact millions of dental patients each year. In fact, the approach is so promising it won second prize in the materials category of the Royal Society of Chemistry’s Emerging Technology Competition for 2016.
Competition entries were judged on the degree of innovation of the technology, its potential impact, and the quality of the science behind it. Increasing innovation in the chemical sciences is a key element of the Royal Society of Chemistry’s industry strategy.
 Effective and practical approach to regenerating teeth
Effective and practical approach to regenerating teeth
The stem cell stimulating filling promises to change the future of dentistry, according to David Mooney, Pinkas Family Professor of Bioengineering at the John Paulson School of Engineering and Applied Sciences at Harvard and the Wyss Institute for Biologically Inspired Engineering.
“’These materials may provide an effective and practical approach to allow a patient to regenerate components of their own teeth,’ Pinkas says.
Stem cells can induce regenerative, self-healing qualities in any tissue found in the body and can, as a result, provide unlimited potential for medical applications. Current studies are underway worldwide to learn how stem cells may be used to prevent or cure diseases and injuries such as Parkinson’s disease, type 1 diabetes, heart disease, spinal cord injury, muscular dystrophy, Alzheimer’s disease, strokes, burns, osteoarthritis, vision and hearing loss, and more. Stem cells may also be used to replace or repair tissue damaged by disease or injury.
###

- Published in Blog
New Guidelines for Stem Cell Research and Therapies Aim to Protect Patients from Charlatan Quackery

Stem cell research has never been more advanced, and as a result many different types of treatments are currently offered on the market. Unfortunate
ly, some providers are practicing quackery in stem cell therapies, and an abundance of well-intentioned scientific and medical personnel are prematurely publicizing their work. These providers and publishers have cast an unfair shadow of mistrust on this very important branch of medical research and potential treatments.
On the other hand, the contributions of professional medical and stem cell societies and other organizations require self-regulation through accreditation and certification, development of standards, and creation of a platform for collaboration among stakeholders.
Professional Guidelines for responsible Stem Cell Research
 International Society for Stem Cell Research (ISSCR) is the largest professional organization of stem cell scientists. In 2007, ISSCR impaneled a broad international taskforce to develop a set of professional guidelines for responsible translational stem cell research. Their principles include high standards of preclinical evidence, peer review, scrupulous review of clinical protocol by an Institutional Review Board (IRB), rigorous informed consent, and publication of results whether positive or negative.
International Society for Stem Cell Research (ISSCR) is the largest professional organization of stem cell scientists. In 2007, ISSCR impaneled a broad international taskforce to develop a set of professional guidelines for responsible translational stem cell research. Their principles include high standards of preclinical evidence, peer review, scrupulous review of clinical protocol by an Institutional Review Board (IRB), rigorous informed consent, and publication of results whether positive or negative.
The general scientific consensus is that most stem cell therapies are not ready for marketing or commercialization. But the industries that are providing these treatments are increasingly sophisticated and organized, and are challenging established regulatory frameworks.
The International Society for Cellular Therapy (ISCT) has an interest in the promotion of stem cell research and development, but it also is interested in a broader range of cell-based interventions such as immune cell interventions, reproductive medicine, and gene therapy. The ISCT taskforce has working groups on definitions, scientific evidence and biological rationale, laboratory cell processing, clinical practice, regulation, commercial implications, communications, and policy.
Develop terminology, define levels of scientific evidence in new guidelines for stem cell research
The key goals are to develop an appropriate terminology, define the levels of scientific evidence needed to justify routine use or commercialization of a stem cell therapy, address questions of “experimental” and “innovative” use, and understand the global regulatory landscape in order to identify gaps and contradictions.
The ISSCR published revised guidelines for research and clinical translation involving stem cells on May 12, 2016. These new guidelines update and combine guidelines on stem cell research and clinical translation previously issued in 2006 and 2008 Jonathan Kimmelman, Associate Professor of Biomedical Ethics at McGill University, chaired the ISSCR Guidelines Update Task Force. The task force was made up of 25 experts in basic research, clinical research, and bioethics, and received feedback from 85 external individuals and organizations.
2016 guidelines: covering new ground in stem cell research
The 2016 guidelines cover new ground in areas such as gene editing and induced pluripotent stem cells. They introduce a new focus on the communication of results. The task force recognizes that results and potential applications can be exaggerated, leading to distorted understandings of research outcomes in the scientific community, popular press, and among potential patients. The “14-day rule” limiting experimentation on human embryos or embryo-like structures is upheld in these guidelines, although one task-force member has suggested that this may soon be open to revision.
In May, 2016 ISSCR released the following list of all of the new topics addressed in the revised guidelines as part of the announcement of its report:
- Define an Embryo Research Oversight (EMRO) process to encompass both human embryonic stem cell research and human embryo research that may not explicitly pertain to stem cells or generating new stem cell lines;
- Exclude the generation of induced pluripotent stem cells (iPS cells) from specific stem cell research oversight, and instead call on the existing human subjects review processes to oversee donor cell recruitment (iPS cells behave like embryonic stem cells but are derived by reprogramming more differentiated tissue cells);
- Support laboratory-based research that entails gene editing of the nuclear genomes of human sperm, egg, or embryos, when performed under rigorous review, but hold that any attempt to apply this clinically would be premature and should be prohibited at this time;
- Define principles for evaluating both basic and clinically applied research on mitochondrial replacement therapy, in concordance with recent deliberations in the U.K., U.S., and elsewhere;
- Determine that where there is no undue financial inducement to participate, it may be acceptable to compensate women who donate eggs for research;
- Recognize that the development of increasingly complex in vitro models of early stages of human development should undergo specialized review;
- Highlight opportunities to strengthen preclinical studies in stem cell research, including reproducibility and stringent standards for experimental design;
- Call for robust standards for preclinical and clinical research evidence as clinical trials progress and rigorous evaluation for safety and efficacy before marketing approval;
- Address the valuable contributions made by patients or patient groups to support clinical research and a framework to ensure this is achieved without compromising the integrity of the research;
- Highlight the responsibility of all groups communicating stem cell science and medicine—scientists, clinicians, industry, science communicators, and media—to present accurate, balanced reports of progress and setbacks.
The good news is that stem cell research is evolving into a highly respected and in-demand branch of healing that many consider to be the future of medicine. Since pluripotent stem cells have the ability to differentiate into any type of cell, they are used in the development of medical treatments for a wide range of conditions including physical trauma, degenerative conditions, and genetic diseases (in combination with gene therapy). Further treatments using stem cells are being developed due to stem cells’ ability to repair extensive tissue damage.
Great levels of success and potential have been achieved from research using adult stem cells. In early 2009, the FDA approved the first human clinical trials using embryonic stem cells. Embryonic stem cells are pluripotent, which means they can become any cell type of the body, with the exception of placental cells. More and more is being discovered about the plasticity of adult stem cells, increasing the potential number of cell types an adult stem cell can become.
###

- Published in Blog
Stem Cell Myths, Busted
The term stem cell research gleans different reactions from people, both in the medical community and the wider public. Still an emerging science, stem cell research is shrouded by many myths and misconceptions. Here, we take on some of the most predominant myths to discuss the misconceptions and clarify the facts regarding this fast-growing branch of medicine.
Myth #1: Stem cells only come from embryos.
FACT: False. Stem cells exist in all bodies, from embryos to adults.
Embryonic stem cells come from the early embryo, and have the potential to produce all the specialized cells of the body. Because of this, they hold great promise for studying and potentially treating disease and injuries. Tissue or “adult” stem cells are found in the body throughout our lives. These cells maintain and repair many tissues in the body. Examples of these cells include blood stem cells, muscle stem cells, bone marrow stem cells, adipose tissue (fat) stem cells and skin stem cells. Some of these adult stem cells are used in established medical and aesthetic treatments.
Myth #2: Induced pluripotent stem cells (iPSCs) eliminate the need for embryonic cells
FACT: False. Research is needed on all types of cells because it is not clear which cells will be most useful for which types of application. For the foreseeable future, side-by-side research on both embryonic and induced pluripotent stem cells is needed. Global Stem Cell Group’s research and treatment products use no embryonic stem cells.
Myth #3: Stem cell research leads to cloning humans.
FACT: False. Most countries prohibit this type of cloning.
In most countries, even attempting to clone a human being is illegal. Some countries do allow something called “therapeutic cloning” for the purposes of studying a disease. In this procedure, scientists isolate embryonic stem cells from a cloned blastocyst (early stage embryo) but do not transfer the blastocyst into a womb. In therapeutic cloning, the blastocyst is not transferred to a womb. Instead, embryonic stem cells are isolated from the cloned blastocyst. These stem cells are genetically matched to the donor organism for studying genetic disease. For example, stem cells could be generated using the nuclear transfer process described above, with the donor adult cell coming from a patient with diabetes or Alzheimer’s. The stem cells could be studied in the laboratory to help researchers understand what goes wrong in diseases like these.
Therapeutic cloning also could be used to generate cells that are genetically identical to a patient’s. A patient transplanted with these cells would not suffer the problems associated with transplant rejection. To date, no human embryonic stem cell lines have been derived using therapeutic cloning.
Myth #4: Adult stem cells are only found in adults
FACT: False. There are three different types of stem cells: embryonic stem cells, induced pluripotent stem cells and tissue specific stem cells. It’s the tissue stem cells that are often called “adult” stem cells, but these “adult” stem cells are found in people of all ages. (See myth #1).
Myth #5: Embryonic stem cell research is banned in Europe.
FACT: False. The laws vary across the EU.

EU member states have diverging regulatory positions on human embryonic stem cell research. For instance, in Germany, the use of embryos for research is heavily restricted under the Embryo Protection Act (Embryonenschutzgesetz) of 1991, which makes the derivation
of embryonic stem cell lines a criminal offense. But in the UK, embryonic stem cell research is allowed, subject to licensing from the Human Fertilization and Embryology Authority (HFEA). Click here for country by country overviews for more details. Under the previous two European Framework programs (FP6 and F7), as well as the current program, Horizon 2020, human embryonic stem cell research can be funded, provided that the work is permitted by law in the country where it is to take place.
Myth #6: Stem cell research and treatment is against the law in the US.

FACT: False. The FDA does not regulate the practice of medicine, but rather drugs and medical devices and which of these can be marketed in the US. Under federal law, cultured (grown) stem cell products are considered a drug, but are not illegal. Adult stem cells, however, are not cultured—they exist in our bodies throughout our organs, blood, skin, teeth, fat, bone marrow and other places.
Adult stem cell therapy is currently used in the United States to treat conditions such as leukemia and other illnesses. Bone marrow consists of stem cells which have been transplanted for years in the US.
Global Stem Cells Group offers stem cell treatments in countries where stem cell therapy is approved and regulated with no appreciable difference in safety record.. Stem cell therapy technology is still under review by the FDA.
Myth #7: Bone marrow is the best source of stem cells.
FACT: False. Bone marrow is just one source of stem cells. Bone marrow stem cells have been studied for decades, and have been used to treat certain types of cancer. A great deal of research has been dedicated to understanding this source of stem cells and their potential. Bone marrow contains a number of different kinds of stem cells, one of which is mesenchymal stem cells. However, mesanchymal stem cells can also be found in adipose (fat) tissue at nearly 2000 times the frequency of bone marrow.
Mesenchymal cells have the capability to become different types of tissues (blood vessels, muscle tissue, etc.) and are capable of communicating with other cells. In combination with other proteins, molecules and regenerative cells found in adipose tissue, they also have the ability to reduce inflammation, regenerate damaged tissue, and grow new blood vessels, a process known as angiogenesis. Stem cells from adipose tissue are more accessible and abundant. They can be processed immediately and reintroduced into the body right away.
Myth #8: There is a risk of rejection with stem cell therapy.
FACT: False. When a patient’s stem cells are derived from his or her own body (such as fat tissue), there is no risk of rejection. In fact, studies thus far have indicated no safety issues with fat-derived autologous (from self) stem cells. Since these stem cells come from your own body, the risk of rejection is eliminated.
###
- Published in Blog
Gordie Howe’s Stem Cell Treatments Support a Growing Appeal for These Therapies Among Athletes and Baby Boomers
In October, 2014, legendary hockey player Gordie Howe, then 86, was on death’s door after suffering a debilitating acute hemorrhagic, left thalamus stroke. Upon returning home from the hospital, Howe needed someone to lift him from his bed to a wheelchair and back. He couldn’t remember the names of his four children, Marty, Mark, Cathy, and Murray, and his condition continued to grow worse in subsequent weeks. According to an article in New York Magazine, when Mark took hid father to get an epidural to relieve his back pain, the attending physician took one look at Gordie and asked Mark if it might be better to just let his father go. On the rare occasion when Gordie did mange to speak, he would tell his children, “Just take me out back and shoot me.”
Howe retired from hockey at age 52, having scored more goals than any other player. But over the past 10 years, his health declined dramatically—heart disease, dementia, and spinal stenosis—despite his family’s and physician’s best efforts to find medical solutions. After his stroke, Keith Olbermann aired a preemptive obituary on ESPN. The family made funeral plans. Murray, his youngest son, wrote a eulogy.
Around Thanksgiving, 2015, Howe’s family learned about an experimental stem cell treatment that could save his life. The plan was to inject up to 100 million neural stem cells into his spinal column in the hopes that the stem cells would migrate to his brain and help his body repair itself. Howe could improve within 24 hours, and receive the treatment anytime—just not in the United States. The procedure wasn’t FDA-approved, and Howe would have to receive the treatment at a clinic in Tijuana.
Howe’s son Murray, a radiologist, looked into the treatment and thought it was promising. The real concern was transporting the immobile Howe to Mexico. Daughter Cathy worried that he might die during the treatment, but Mark responded bluntly: “If he does die, what’s the difference? He’s going to be gone soon no matter what.”
While the family weighed the stem cell treatment idea, Howe was admitted to the hospital with severe dehydration, caused by his unwillingness to swallow. When he returned home, he still had no use of his right side, and the family

Gordie Howe, mid-career
assumed he would never walk again. The Howe children decided to give the stem cell treatments a try.
Two days later, the Howes flew their Dad to San Diego. In the air, Gordie grew agitated and got the attention of a flight attendant, who spent 10 minutes kneeling by his seat trying to understand something he wanted to tell her. Due to his profound memory loss, Howe didn’t know he had suffered a stroke, why he was on a plane, or where he was going. But he remembered one thing, which he managed to whisper to the fight attendant: “I was a pro hockey player.”
The next morning, Marty and Murray drove with their father across the border to Clínica Santa Clarita, where Gordie bent over a table to expose his lower back so that a needle could be inserted into his spinal canal to inject the stem cells. Howe was given two types of stem cells – neural stem cells and mesenchymal stem cells. The second type, derived from bone marrow, has anti-inflammatory properties and secretes chemicals that promote healing.
The procedure then required Howe to lie prone for eight hours. After the eight hours passed, Gordie told Murray he needed to use the bathroom and that he intended to walk there in order to do so. Since the stroke, Gordie had only managed to walk one time—10 steps, with a walker. Murray reminded his Dad that he couldn’t walk.
Howe stood up, and with Murray’s support, walked for the first time in more than a month—to the bathroom. This milestone became an oft-repeated story among the Howe family, and Gordie’s revival became an irresistible story for the sports pages. Back home, Gordie returned to something resembling the normal life of an 86-year-old. He pushed the grocery cart, helped with the dishes, and could go fishing so long as one of his sons reminded him that a tug on the line meant he needed to start reeling. The family released a video of Gordie standing stationary, firing a puck, five-hole, past his 8-year-old great-grandson. Keith Olbermann apologized for his premature obituary.
Howe’s children now had to figure out how to share his apparent recovery—a debate that proved just as contentious as their decision to fly him to Mexico for the treatment in the first place—with the world. Both Marty and Mark had played in the NHL alongside their father, but now Murray, the doctor, was giving interviews in his hospital scrubs, endorsing his father’s place in medical “miracle” history. He began referring to the stem-cell treatment as the “Gordie Howe Protocol,” and said that his Toledo-based hospital was looking into conducting an FDA-approved study of the procedure. In one interview, Murray Howe stated that “stem cells are the most promising thing in medicine since the discovery of antibiotics.”
As the story spread, the medical community started to question just how miraculous Howe’s recovery had been.
“Companies selling these products are preying on desperate and vulnerable people and exploiting their hope, much like snake-oil salesmen have done throughout most of human history,” wrote Judy Illes and Fabio Rossi, stem-cell experts at the University of British Columbia, in the Vancouver Sun. Even advocates pointed out that, though the field holds great promise, no reputable studies have shown that such a procedure should work.
And yet, for the children of ailing parents, such skepticism doesn’t matter. Murray’s response to one skeptic was, “What would you do for your father?”
Gordie Howe’s therapy, would cost an average patient about $30,000.
Athletes, whether playing or retired, have a special need for the regenerative capacity that stem cells are believed to provide. Athletes break bones, strain ligaments, bash knees and wear out cartilage. If stem cells’ restorative capability is proven, they could be considered the latest form of sports medicine.
Since Howe’s treatment in late 2014, two other athletic legends have received stem cell treatments—former quarterbacks Bart Starr and John Brodie. And the rest of the population, particularly aging baby boomers, isn’t far behind.
Still, while accepta
 nce of stem cell therapy has grown, so have controversies surrounding its use. While clinical trials authorized by the U.S. Food and Drug Administration are rapidly expanding in the U.S., so are treatments outside the regulated system. Patients are going to stem cell clinics in other countries that approve stem cell therapies.
nce of stem cell therapy has grown, so have controversies surrounding its use. While clinical trials authorized by the U.S. Food and Drug Administration are rapidly expanding in the U.S., so are treatments outside the regulated system. Patients are going to stem cell clinics in other countries that approve stem cell therapies.For its part, the FDA is drafting guidelines, although the U.S. and Canada still trail other countries in approving stem cell treatments.
Last year, the FDA issued draft guidelines to clarify what types of human cell therapy it regulates. The short answer: Most of them, with “limited exceptions,” according to an FDA email sent in response to questions from The San Diego Union-Tribune. These exceptions include cells or tissues that are “minimally manipulated,” not given with any other product and perform the same function in the donor as in the recipient.
All other stem cell therapies are seen as involving human cells, tissues and cellular and tissue-based products – also known as HCT/Ps – regulated by the FDA’s Center for Biologics Evaluation and Research.
“We understand that determining the appropriate regulatory path for HCT/Ps can be challenging, and the FDA is working diligently to develop guidance to help sponsors and physicians understand how to apply federal regulations to this complex and emerging field,” the agency said.
In January 2015, University of California, Davis stem cell researcher and blogger Paul Knoepfler estimated that more than 100 unauthorized stem cell clinics were operating in the United States. Later that year, he increased that estimate to up to 200.
Then on May 6, he wrote on his blog: “We are seeing a flood of professional athletes getting stem cell treatments in the past few years.”
Athletes and others who want these treatments bristle at what they call cumbersome, time-consuming regulations in the U.S. The situation can be urgent for seriously ill patients.
While it hasn’t been proven that the stem cells enabled his recovery, by all indications Gordie Howe’s health has improved significantly since receiving stem cell treatments. In November, 2015, Murray Howe said that his father’s physicians in the U.S. recommended hospice care in the weeks after the stroke, and the family was told he wouldn’t last more than two or three weeks,
“Then, suddenly, he is raking and sweeping and goofing around in the back yard,” Murray said.
###
Sources: The San Diego Union-Tribune, New York Magazine
- Published in Blog
Stem Cell Researchers Discover Stem Cells That Might Repair Skull, Face Bones
Scientists may be one step closer to a breakthrough that uses stem cells to replace damaged skull and facial bones in patients who experience a head trauma or undergo cancer surgery requiring repair and reconstructive surgery.
Researchers have discovered and isolated stem cells capable of repairing these bones in mice. The research, led by Takamitsu Maruyama and the research team at the University of Rochester Medical Center in Rochester, N.Y., could also help patients born with a skull deformity known as craniosynostosis, which can lead to developmental delays and pressure on the brain.
 In the study, scientists investigated the role of the Axin2 gene in bone formation and regeneration. They also examined a specific mutation that causes craniosynostosis in mice. Their finding show that stem cells involved in skull formation are contained within this cell population. These cells are specificto the bones in the head and are very different from other stem cells involved in the formation of the bones in the legs and other parts of the body.
In the study, scientists investigated the role of the Axin2 gene in bone formation and regeneration. They also examined a specific mutation that causes craniosynostosis in mice. Their finding show that stem cells involved in skull formation are contained within this cell population. These cells are specificto the bones in the head and are very different from other stem cells involved in the formation of the bones in the legs and other parts of the body.
Tests to uncover these cells could also help physicians detect bone diseases caused by stem cell abnormalities, according to the researchers.
The research was published Feb. 1 in the journal Nature Communications.
- Published in Blog
Our Friend MSCs (Mesenchymal Stem Cells)—Bringing New Life to Old Bones
Researchers from the University of Toronto and The Ottawa Hospital were looking to see if mesenchymal stem cells (MSCs) might treat osteoporosis. MSCs are multipotent stromal cells that can differentiate into a variety of cell types, including: bone cells (osteoblasts), cartilage cells (chondrocytes), muscle cells (myocytes) and fat cells (adipocytes).
Faulty MSCs are the culprits behind osteoporosis; after injecting healthy MSCs into mice with the affliction that causes bones to become weak and brittle, researchers were hoping for a general increase in the mice’s bone health. Instead, they were surprised (and probably very excited) to discover after six months—a quarter of a mouse’s life span—that healthy, functioning bone had replaced the damaged osteoporotic bone. The bone structure in the little creatures, which had been severely compromised by osteoporosis, had been restored to a normal, healthy state! The healthy mesenchymal stem cells did what they were born to do. They became bone cells and went to work, much like the restoration of an old building at the hands of architects and laborers, only without the scaffolds and noise. MSCs work very quietly.
Researchers are hoping that these findings could lead to a new way of treating osteoporosis in humans, or even delay its onset indefinitely.
Stem cell researchers have known for some time that MSCs can boost the regeneration of bone, and in fact a test group of elderly patients in the U.S. who suffer from osteoporosis have already received MSC injections as part of an ancillary trial. The research team is preparing to to examine their blood samples to see if biological markers indicate an improvement in bone growth and bone reabsorption.
Depending on the outcome of those blood tests, larger trials involving human patients could follow within the next 5 years.
In addition to working quietly and therefore not waking you to the sound of a jackhammer at 7 a.m., there are other cool qualities to MSCs. For instance, they are “a heterogeneous population of musculoskeletal progenitors (another name for adult stem cells) that includes skeletal stem cells (SSCs).” An added perk is that they can be transplanted between individuals without the need to be matched, and without the risk of rejection.
MSCs are awesome.
Globally, more than 200 million people are living with either postmenopausal osteoporosis—known as type 1 osteoporosis, which affects mainly women, or age-related type 2 osteoporosis, which affects both men and women.
With type 2 osteo porosis, there is a reduction in the inner structure of the bone. The bone becomes thinner and less dense, and it can no longer function properly.
porosis, there is a reduction in the inner structure of the bone. The bone becomes thinner and less dense, and it can no longer function properly.
Worldwide, type 2 osteoporosis leads to around 8.9 million bone fractures annually. Hip fractures are among the most common fractures related to osteoporosis, which can lead to disability and even death in elderly patients.
Currently, Teriparatide (brand name Fortéo) is the only drug available to treat type 2 osteoporosis, and its effectiveness lasts for only two years.
The senior author of the study, titled Systemic Mesenchymal Stromal Cell Transplantation Prevents Functional Bone Loss in a Mouse Model of Age-Related Osteoporosis, and published March 17, 2016, is William Stanford, Ph.D., a senior scientist at The Ottawa Hospital Research Institute and a professor at the University of Ottawa. Previous research led Stanford to discover the association between defects in MSC and age-related osteoporosis in mice.
The study’s co-author, John E. Davies, Ph.D., D.Sc., is a professor at the University of Toronto’s Institute of Biomaterials and Biomedical Engineering, The study’s findings are published in the current issue of Stem Cells Translational Medicine.
- Published in Blog
