Culture Expanded MSCs

Mesenchymal Stem Cells (MSCs) are the most commonly used cells in stem cell therapy and regenerative medicine, due to their high and multi-potency. Mesenchymal Stem Cells (MSCs) can be isolated from different tissues in the body.
In this article, you’ll be learning about culture-expanded MSCs, how MSCs can be expanded, The potency of MSCs and the type of cells they can differentiate into.
What are culture expanded Mesenchymal Stem cells?
Mesenchymal stem cells are high potent cells used for cellular therapy and isolated from different parts of the body. Mesenchymal stem cells can be used to improve the patient outcome in diseases and conditions such as autoimmune diseases, degenerative diseases, nerve damage, diabetes mellitus, bone problems etc.
For every patient, millions of mesenchymal stem cells are needed and the exact amount varies according to disease, route of administration, administration frequency, weight, and age of patient.
Mesenchymal stem cells are expanded in a culture media, on a large scale in order to obtain the required quantity of cells needed for cellular therapy.
Culture expanded MSCs: How does it work?
Expanding Mesenchymal stem cells in a media involves step by step process of isolation and expansion.
Mesenchymal Stem Cells Isolation
Mesenchymal stem cells can be isolated from different tissues in the human body such as adipose tissues, dental pulp, human bone marrow, umbilical cord tissue, umbilical cord blood, peripheral blood and synovium.
Mesenchymal stem cells are expanded in culture to increase their yield and amplify their desired functions and potency.
Although the population of Mesenchymal Stem Cells obtained will vary from donor to donor, here are some steps to follow:
· Acquire fresh tissue extracts in strictly aseptic conditions, to maintain purity.
· To remove any cell clusters, you have to filter the cell suspension with a 70-mm filter mesh
· Use a centrifuge to roll the cells for about 5 minutes at 500g
· Suspend the cells again the cells to measure the cell viability and yield using Trypan blue exclusion
· Use in T75 culture dishes to culture the cells in 10 mL of complete MSC medium at a density of 25 × 106 cells/mL. You can then go on to Incubate the plates at 37 °C with 5% CO2 in a humidified chamber without any interruption.
· When it’s past 3 h, remove the non-adherent cells that accumulate on the surface of the dish by changing the medium and replacing it with 10 mL fresh complete medium.
· After an additional 8 h of culture, add 10ml fresh complete medium as a replacement for the existing medium. You’ll have to repeat this step every 8 h for up to 72 h of initial culture.
· Cells can be frozen in MSC growth media plus 10% DMSO (D2650) at a density of 2X106 cells/vial.
Expansion of Mesenchymal Stem Cells in a culture media
Culture expanded mesenchymal cells undergo various stages from the preparation of the culture plate, thawing of Mesenchymal stem cells, and the actual expansion of Mesenchymal stem cells.
The reason behind the cultural expansion of Mesenchymal stem cells is to get them to differentiate into other cell types such as osteoblast, adipocyte, and mesenchymal stromal cells.
In preparation, to expand MSCs in a culture media, you need a culture ware. You can get one plastic or glassware plate and coat it with a sufficient amount of 0.1% gelatin. Don’t forget to aspirate the gelatin solution from the coated plate or flask before you use it.
The next step involves the thawing of the Mesenchymal stem cells, and here are a few steps for you to follow:
After the recommended culture medium and coated culture ware is ready and on standby, remove the vial of Mesenchymal Stem Cells from liquid nitrogen and incubate in a 37C water bath and pay close attention to it, until all the cells are completely thawed. The extent of completely thawed frozen cells and how fast, are what determines the cell viability.
Once the cells have thawed completely, take steps to avoid contamination by disinfecting the walls with 70% ethanol, before you proceed to the next step.
Place the cells in a hood, and carefully transfer the cells to a sterile tube with a pipette (1 or 2ml pipette), Do this in such a way to prevent bubbles.
Then, add drops of Mesenchymal Stem cell expansion medium that have been pre-warmed to 37C to the tube containing the Mesenchymal stem cells.
Be careful to take your time when adding the medium to avoid osmotic shock which could lead to decreased viability.
Proceed to mix the suspension slowly by pipetting up and down two times while avoiding any bubbles.
Place the tube in a centrifuge and centrifuge the tube at 300 x g for 2-3 minutes to roll the cells, and you should not vortex the cells.
After this, then decant as much of the supernatant as possible. These steps are necessary to remove residual cryopreservative (DMSO).
Suspend the cells in a total volume of 10 mL of Mesenchymal Stem Cell Expansion Medium again or any alternative of choice, pre-warmed to 37 °C, containing freshly added 8 ng/mL FGF-2 (F0291).
The next step involves placing the cell suspension onto a 10-cm tissue culture plate or a T75 tissue culture flask.
Maintain the cells in a humidified incubator at 37 °C with 5% CO2.
The next day, exchange the medium with fresh Mesenchymal Stem Cell Expansion Medium (pre-warmed to 37 °C) containing 8 ng/mL FGF-2*. Replace with fresh medium containing FGF-2 every two to three days thereafter.
Isolate the cells when they are approximately 80% confluent, using Trypsin-EDTA and passaged further or frozen for later use.
Expansion of Mesenchymal Stem Cells
Once the cells are actively proliferating and have reached a confluence of approximately 80% (before 100%), you should subculture the cells.
Then remove the medium from the 10-cm tissue culture plate containing the confluent layer of human mesenchymal stem cells, carefully and apply 3-5 mL of Trypsin-EDTA Solution, before proceeding to incubate in a 37 °C incubator for 3-5 minutes.
Crosscheck the culture to see if all the cells are completely detached. Then, add 5 mL Mesenchymal Stem Cell Expansion Medium to the plate.
Swirl the plate mildly to mix the cell suspension. Transfer the separated/isolated cells to a 15 mL conical tube.
Centrifuge the tube at 300 x g for 3-5 minutes to pellet the cells.
Throw the supernatant away and apply 2 mL Mesenchymal Stem Cell Expansion Medium (pre-warmed to 37 °C) containing 8 ng/mL FGF-2 to the conical tube and completely suspend the cells again. Remember not to vortex the cells.
Then, use a hemocytometer to count the number of cells.
Plate the cells at a density of 5,000-6,000 cells per cm2 into the appropriate flasks, plates, or wells in a Mesenchymal Stem Cell Expansion Medium containing 8 ng/mL FGF-2.
Cells can be frozen in MSC growth media plus 10% DMSO (D2650) at a density of 2X106 cells/vial.
Functions of Culture Expanded MSCs
Mesenchymal stem cells are required to be expanded in order for them to be used clinically for therapeutic purposes.
The culture expanded MSCs can be induced to differentiate into adipocytes, osteocytes, hepatocytes, chondrocytes, tenocytes and cardiomyocytes.
Because of its potential to differentiate into different kinds of cells in the body, it can be used to manage liver problems, heart problems, joint and bone problems etc.
Mesenchymal stem cells are also used in tissue regeneration and modulation of the immune system. They possess anti apoptotic, angiogenic, anti fibrotic, and anti-oxidative properties.
However, the quantity of MSCs isolated from body tissues is not enough for clinical and therapeutic applications.
This is why MSCs are expanded in culture to increase their yield for desired therapeutic effect.
- Published in Blog
Why cellular therapies have become a standard in clinics that are betting on biological medicine

Cellular therapy is fast becoming a standard therapy in many regenerative clinics today. Many doctors are no longer questioning the safety and effectiveness of stem cell therapy. This is because various stem cell studies are already describing the benefits of stem cells for patients who are living with chronic and autoimmune health conditions.
This article will be talking about why stem cell therapy have become a standard therapy in clinics, the paracrine effect of stem cells, and other reasons why doctors are adopting stem cells in their clinics.
Benefits of stem cell therapy
Stem cell therapy is an important innovation in medicine because of its regenerative power in the human body. Most disease states are characterized by damaged cells, tissues and organs, which is where stem cell therapy comes in. In stem cell therapy, stem cells are administered into the human body and it replaces the cells damaged by disease or health disorders.
Stem cell research has revealed two major ways of using stem cells to rebuild defective and damaged cells. One of these ways can be seen in procedures like bone marrow transplant, where stem cells are used to replace the damaged cells by engraving, and they then differentiate into the proper cell type. Another mechanism relies on the paracrine effect of stem cells. This procedure of stem cell therapy involves using stem cells isolated from a donor to stimulate the patient’s cells to repair damaged tissues.
Additionally, unlike traditional therapy, stem cells have a wide application. Stem cell therapy is used to manage various degenerative diseases, autoimmune disorders, birth defects, and the research is still ongoing for so many other health conditions where stem cells have shown potential.
Also, there is currently a high demand for aesthetic medicine. Stem cell therapy is a proven alternative to other forms of cosmetology such as plastic surgery. Hence, dermatologists are turning to stem cell therapy to administer anti-aging procedures, skin rejuvenation, hair therapy, micro-needling etc.
The Paracrine effect of stem cells
The paracrine effect of stem cells is one of the most outstanding effects of stem cells. It involves using donor cells to stimulate endogenous repair by harnessing the regenerative power of the human body. It is a mechanism of tissue regeneration that has created new possibilities for managing various conditions using stem cell therapy.
The cells that trigger a paracrine response are; mesenchymal cells, umbilical cord blood, umbilical cord tissue, adipose (fat) tissue and blood cells from a donor’s bone marrow.
The paracrine effect occurs when the donor’s cells send the damaged or defective cells signals to induce self regeneration and repair by secreting some factors and proteins. One of the mechanism by which this paracrine effect is initiated, involves the secretion of cytokines and regulatory proteins by the damaged patient’s cells, these cytokines and proteins act as mediators to stimulate an immune response that attracts the donor cells, this causes the donor cells to release proteins and factors that stimulate the patient’s cells to promote cell proliferation, increase vascularization and blood flow to the areas that needs to heal, while reducing inflammation.
Moreover, research has shown that the paracrine effect of stem cells prevents damaged and diseased cells from dying. They are also therapeutically useful in autoimmune diseases and preventing transplant rejection due to the immune suppression effect they have.
Is stem cell therapy effective?
Doctors are always looking for ways to provide the best possible treatment to their patients, and that is why many clinics are embracing stem cell therapy as a standard, due to its many advantages.
Stem cell therapy is one of the most effective and safest therapy patients can receive, when compared to other existing treatment options. Stem cell therapy is used in promoting patient outcomes in a lot of disease conditions that were previously poorly treated by other alternatives.
Again, as new potentials and ways of applying stem cells are being discovered, doctors are beginning to maximize these benefits in their clinics. Some conditions that are currently treated by stem cells include autoimmune conditions, immunotherapy Car-T cells, chronic obstructive pulmonary disease, neurodegenerative conditions, osteoarthritis, spinal cord injury, aesthetics/anti-aging, sports medicine, autism and multiple sclerosis.
Another reason clinics are adopting stem cell therapy as a standard therapy is because it is easy to administer. A lot of machines such as GCELL which makes the harvesting and processing of stem cells easy and fast, have made the procedures easily adaptable by doctors.
Furthermore, stem cell therapy reduces the treatment and recovery time associated with surgical procedures and other treatment options. This alone is a big factor in why stem cells are becoming a standard therapy in clinics.
Therapeutic uses of stem cells vs traditional medicine
Existing stem cell research has shown how the regenerative effect of stem cells is defining the future of medicine. The major advantage of stem cell therapy over conventional medication-based therapy is its safety. Stem cell therapy is aimed at treating the cause of the disease while traditional medicine targets the symptoms.
Another problem with traditional medical therapy is that it introduces another problem while trying to solve the existing one. As a doctor, you always run the risk of causing harm with each prescription because of various adverse effects that could lead to major organ damage of the kidney, liver etc. On the other hand, patients already know this and they are actively seeking better alternatives, this is why stem cell therapy is fast becoming a standard therapy in clinics.
Moreover, doctors will always be concerned about whether their patients are taking their medications or not. The burden of drug compliance and adherence associated with traditional medical therapy is not always easy to navigate. This is why effective treatment options like stem cell therapy have become a standard therapy in clinics. It only requires the patients having a procedure that repairs and restores damaged cells and tissues in the most natural way.
If you would like to become certified in regenerative medicine using stem cells and other cellular therapy, contact us.
- Published in Blog
Exosome Therapy – The Secret Treatment of Anti-Aging

Overview – The Secret Treatment of Anti-Aging
Over the past few years, exosomes had made a name in the field of rejuvenation and antiaging. Based on the available data, it seems that exosomes will be an integral part of rejuvenation therapy, especially in people interested in stem cell therapy.
Unsurprisingly, many people have never heard of exosomes. So, what exactly are exosomes? How would they help with aging? And what is the difference between exosome therapy and stem cell therapy?
In this article, we will answer all of these questions to help you understand the potential role of this innovative technique.
What are exosomes?
Inside your cells, there are several components that serve different functions. We call them organelles. When these components fuse with the membrane of the cell, exosomes form.
Close inspection of these exosomes shows that they contain protein, lipids, RNA, and other elements of the hosting cell.
Using this complex physiological concept, researchers used stem cell-derived exosomes to repair different tissues. The unique blend of components found inside of these vesicles makes exosomes very effective in boosting the body’s own regenerative ability.
Moreover, exosomes help with getting rid of cytotoxins, making them very effective in dampening chronic inflammation.
How will exosome therapy help your skin
As we age, our skin becomes prone to age-related deterioration, such as wrinkles. Primarily, these issues originate when you can’t regenerate the lost components of your skin.
The good news is that exosomes might just be the solution you’ve been looking for. This treatment will delay the aging process and promote skin regeneration.
When studied in the laboratory, exosomes showed some impressive effects in delaying the onset of skin aging. Researchers found that this therapy boosts the development of fibroblasts, which are a special type of cells that ensure your skin’s structural integrity and elasticity.
Today, the topical use of exosome therapy can be a fantastic way to slow down the dermatological effects of aging.
Perhaps the best thing about exosomes is the fact that there is no risk of rejection since they are not real tissues but rather a trigger for your own tissues to heal themselves.
What is the difference between stem cell therapy and exosomes?
Stem cell therapy revolves around using whole cells to replace lost tissue. Conversely, exosomes are vesicles that detach from the cells. The way that exosomes help with rejuvenation is by helping other cells using the components carried in the vesicles.
Another key difference between stem cells and exosomes is that the former is only obtained from specific areas of the body, such as:
- Bone marrow
- Blood
- Fat tissue
On the other hand, you can get exosomes from all types of cells.
Takeaway message
The use of exosomes in the field of rejuvenation therapy revealed very promising results in preliminary research studies. If used properly, the clinical applications of this technique could be vast, extending beyond esthetic aspects.
We hope that this article helped you appreciate the role of exosome therapy in addressing the aging process.
Learn more about exosome therapy and the possibility to receive it in Cancun, México by clicking on this link.

- Published in Blog
The Potential Benefits of Stem Cells for Concussions – What You Need To Know (2021)

Overview
Traumatic brain injuries (TBI), also known as concussions, are among the most frequent causes of death in the United States.
According to the Centers for Disease Control and Prevention (CDC), the number of emergency department visits related to TBI admissions, complications, and deaths increased by 53% in recent years.
People who can recover from TBI may experience irreversible neurological issues throughout their lives. As a result, they lose their autonomy and become reliant on other people to perform daily activities.
However, it’s not all doom and gloom. A few studies suggest that stem cell therapy could be beneficial in the management of TBI.
In this article, we’ll discuss everything you need to know about the potential effects of stem cell therapy in managing concussions.
How can stem cells help with concussions
For those unfamiliar with how stem cells function, here is a short description:
Stem cells can develop into any kind of tissue or cell, including those that don’t typically regenerate (e.g., heart cells, nerve cells). For instance, medical schools often teach that a person has the same number of neurons from the moment they are born to their death.
Although this assertion is not completely true due to the latest evidence that supports the ability of neurons to regenerate, the rate of regeneration is nowhere near enough to restore the damaged tissues caused by TBI or strokes.
To this end, researchers are using stem cells to create new neurons to help patients with TBI, multiple sclerosis, and other neurological disorders.
What is the scientific consensus on stem cell therapy and traumatic brain injuries?
Mesenchymal stem cells derived from the bone marrow, umbilical cord, or adipose tissues showed positive results in the management of concussions.
In a number of studies, the administration of stem cell therapy via the spinal cord showed real evidence of lesion improvement. Researchers used advanced imaging techniques such as functional MRI to objectify the changes.
Neuroscientists theorize that stem cells can replace the dead neurons, which helps with restoring some of the lost functions.
Today, hundreds of clinical trials are trying to unveil the full extent of how stem cell therapy helps with traumatic brain injuries.
Based on the available research, scientists advocate for the use of stem cell therapy in treating patients with severe concussions.
However, neuroscientists insist that stem cell therapy is only used in patients who failed to respond to conventional treatment methods.
To see whether you are a candidate for stem cell therapy, contact us by clicking on this link. You will speak with one of our healthcare professionals in Cancun, México.

Takeaway message
Stem cells have an amazing ability to divide into any type of tissue and potentially restore lost functions.
We hope that this article managed to highlight the potential role of stem cell therapy in addressing traumatic brain injury.
If you have any questions or concerns regarding stem cell therapy or TBI, please do not hesitate to share your thoughts in the comment section below.
- Published in Blog
Wharton’s Jelly – how does it work?

Wharton’s Jelly Treatment
Wharton’s Jelly is the substance that helps lubricate and support the umbilical cord. What makes Wharton’s Jelly so special is it contains high levels of mesenchymal stem cells. These special stem cells adapt to fit the cells needed to help regenerate damaged tissue and relieve pain naturally.
The mesenchymal stem cells that come from Wharton’s Jelly contain the most potent stem cells that are rich in regenerative properties. Wharton’s Jelly also contains a good amount of collagen, hyaluronic acid, and anti-inflammatory properties. This makes them quintessential in regenerative medicine.
Regenerative medicine refers to treatments and medicine that is naturally occuring, stem cell therapies being included. Mesenchymal stem cells are harvested from the Wharton Jelly found in the umbilical cord that has been donated by a healthy mother of a full term baby. These stem cells contain all the regenerative properties needed to help the body heal and relieve pain naturally.
How does this treatment work?
Mesenchymal stem cells are injected into the body and have the ability to transmute into cells that are needed to repair damaged tissue and relieve inflammation. These cells harness the potent regenerative properties that help rebuild the injured part of the body and provide long lasting natural pain relief. Unlike pain medicines which provide temporary relief that mask the symptoms and are harmful to the body if taken long term, the stem cells found in Wharton’s Jelly are naturally occurring and natural to the body.
What is Wharton’s Jelly best used for?
Wharton’s Jelly is best used in patients with degenerative diseases and musculoskeletal injuries. The anti-inflamatory and regenerative properties go to work at repairing damaged tissues. Repaired tissue means lasting pain relief and restored function.
What can someone expect?
Once a patient and doctor have decided on this type of stem cell treatment, patients can expect a relatively painless process. Stem cells are injected into the site and immediately go to work. Injections are virtually painless and there are no known negative side effects. Patients can generally get right back to the activities they love. Doctors will discuss treatment plans based on individual needs and in some cases resting an injured area for a particular period of time will be needed.
The mesenchymal stem cells found in Whorton’s Jelly have proven to be a very successful therapeutic method to treat a number of degenerative issues and injuries. This therapy is relatively painless, with no known negative side effects making it an excellent choice in treatment. Instead of masking the pain with dangerous medicine, stem cell therapy offers a naturally occurring solution that aims to repair the damaged tissue and resolve the problem.
If you want to learn more about Wharton’s Jelly Treatment and how can you help your patients, you can check our next training course here
- Published in Blog
Global Stem Cells Group has Announced an Agreement with Rokit Healthcare

Global Stem Cells Group announces an agreement with the South Korean biotechnology giant known as Rokit Healthcare to represent the company’s technology in the Latin American market.
The Global Stem Cells Group (GSCG) a world leader in Regenerative Medicine Technologies has signed an agreement with South Korean-based Rokit Healthcare, an esteemed bioprinter manufacturer that is committed to advancing the field of regenerative medicine and bettering the quality of life of people around the world.
The field of bioprinting is an extremely new one, but it shows great promise. Simply, it is the automated, computer aided deposition of bio-materials (which are cells, growth factors, and biocompatible polymers) for the manufacturing of functional human tissues or organs. Growth factors are harvested and used with a proprietary printing technology to create or regenerative damaged or diseased organs. Rokit Healthcare does this primarily through the proliferation of a machine that they dub an ‘organ regenerator’– it looks like a 3D printer, but instead of using plastics to create things, they use cells and materials that will be safe to implant within the human body.
The process of 3D bioprinting human tissues and organs is a revolutionary technology in the field of tissue engineering. One of the major challenges in regenerative medicine research and tissue engineering is mimicking the micro and macro environment of human tissues. In response to this challenge, advances in additive manufacturing have inspired scientists in Korea to develop novel bioprinting technology, for human tissues and organs
With the advancements of 3D printing and regenerative medicine working together, the potential is seemingly limitless for the spreading of bioprinting technology, a process that is known as 4D Printing– and Global Stem Cells Group, in an effort make this revolutionary technology available to patients, has forged an agreement with Rokit Healthcare to promote, and distribute the company’s technology in Latin America-
The Invivo 4D Printer is Rokit Healthcare’s flagship product, and it is one that revolutionizes the application of regenerative medicine and growth factor-based therapies. creating a solution for personalized and improved patient care. By leveraging a combination of 3D and bioprinting technologies, it can better distribute a patient’s autologous tissues and cells, making it an invaluable tool for those that are looking to improve the efficacy of their results, especially for certain dermatological conditions including scarring.
“We’re extremely excited about this new opportunity and look forward to working with Rokit,” Says Benito Novas, CEO of the Global Stem Cells Group, “The Invivo 4D Printer is in a position to turn the practice of regenerative medicine onto its head, and we are planning on creating a training center in Cancun, Mexico exclusively to showcase and instruct other physicians in this cutting-edge technology,”
About Global Stem Cells Group
Global Stem Cells Group (GSCG) is a worldwide network that combines seven major medical corporations, each focused on furthering scientific and technological advancements to lead cutting-edge stem cell development, treatments, and training. The united efforts of GSCG’s affiliate companies provide medical practitioners with a one-stop hub for regenerative medicine solutions that adhere to the highest medical standards.
Global Stem Cells Group is a publicly traded company operating under the symbol MSSV.
https://finance.yahoo.com/quote/mssv/
About ROKIT :
ROKIT Healthcare is a global healthcare company that is committed to providing an effective and autologous organ regeneration platform. In order to undertake this daunting task, the company uses proprietary biofabrication technologies that show promise in treating several types of diseases in the field of regenerative medicine. Through the proliferation of 4D bioprinting technology, autologous stem cell technologies, ROKIT Healthcare believes that supplying an avenue for organ regeneration will drastically change the way that everyday people trust and manage their own body.
- Published in News
Conventional and novel stem cell based therapies for androgenic alopecia

Dodanim Talavera-Adame,1 Daniella Newman,2 Nathan Newman1
1American Advanced Medical Corp. (Private Practice), Beverly Hills, CA,
2Western University of Health Sciences, Pomona, CA, USA
Abstract
The prevalence of androgenic alopecia (AGA) increases with age and it affects both men and women. Patients diagnosed with AGA may experience decreased quality of life, depression, and feel self-conscious. There are a variety of therapeutic options ranging from prescription drugs to non-prescription medications. Currently, AGA involves an annual global market revenue of US$4 billion and a growth rate of 1.8%, indicating a growing consumer market. Although natural and synthetic ingredients can promote hair growth and, therefore, be useful to treat AGA, some of them have important adverse effects and unknown mechanisms of action that limit their use and benefits. Biologic factors that include signaling from stem cells, dermal papilla cells, and platelet-rich plasma are some of the current therapeutic agents being studied for hair restoration with milder side effects. However, most of the mechanisms exerted by these factors in hair restoration are still being researched. In this review, we analyze the therapeutic agents that have been used for AGA and emphasize the potential of new therapies based on advances in stem cell technologies and regenerative medicine.
Introduction
The prevalence of androgenic alopecia (AGA) increases with age, and is estimated to affect about 80% of Caucasian men.1 Female AGA, also known as female pattern hair loss, affects 32% of women in the ninth decade of life.2 The consumer market for products that promote hair growth has been increasing dramatically.3 These products promote hair regeneration based on the knowledge about the hair follicle (HF) cycle.4,5 However, in most cases, the mechanisms of action of these products are not well characterized and the results are variable or with undesirable side effects.6 At present, only two treatments for AGA have been approved by the US Food and Drug Administration (FDA): Minoxidil and Finasteride.7–10Although these medications have proved to be effective in some cases, their use is limited by their side effects.11,12 With the emergence of stem cells (SCs), many mechanisms that lead to tissue regeneration have been discovered.13 Hair regeneration has become one of the targets for SC technologies to restore the hair in AGA.14 Several SC factors such as peptides exert essential signals to promote hair regrowth.15,16 Some of these signals stimulate differentiation of SCs to keratinocytes which are important for HF growth.17 Other signals can stimulate dermal papilla cells (DPCs) that promote SC proliferation in the HF.18,19 In this review, we describe HF characteristics and discuss different therapies used currently for AGA and possible novel agents for hair regeneration. These therapies include FDA-approved medications, non-prescription physical or chemical agents, natural ingredients, small molecules, biologic factors, and signals derived from SCs.
HF and SC niche
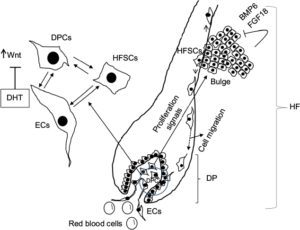
The HF undergoes biologic changes from an actively growing stage (anagen) to a quiescent stage (telogen) with an intermediate remodeling stage (catagen).4 HFSCs are located in the bulge region of the follicle and they interact with mesenchymal SCs (MSCs) located in the dermal papilla (DP).18 These signal exchanges promote activation of some cellular pathways that are essential for DPC growth, function, and survival, such as the activation of Wnt signaling pathway.19–21 Other signals, such as those from endothelial cells (ECs) located at the DP, are also essential for HF maintenance.22 EC dysfunction that impairs adequate blood supply may limits or inhibits hair growth.22 For instance, Minoxidil, a synthetic agent, is able to promote hair growth by increasing blood flow and the production of prostaglandin E2 (PGE2).7 It has been shown that proteins that belong to the transforming growth factor (TGF) superfamily, such as bone morphogenetic proteins (BMPs), also exert signals to maintain the capacity of DPCs to induce HF growing in vivo and in vitro.23 These BMPs may be released by several cells that compose the follicle, including ECs.24–26 ECs may provide signals for BMP receptor activation in DPCs similar to those signals that promote survival of MSCs in human embryoid bodies composed of multipotent cells.24,25 DPCs have been derived from pluripotent SCs in an attempt to study their potential for hair regeneration in vitro and in vivo.27 Together, dermal blood vessels and DPCs orchestrate a suitable microenvironment for the growth and survival of HFSCs.28,29 Interestingly, the expression of Forkhead box C1 regulates the quiescence of HFSCs located in the bulge region (Figure 1).30 HFSCs are quiescent during mid-anagen and maintain this stage until the next hair cycle.29,30 However, during early anagen stage, these cells undergo a short proliferative phase in which they self-renew and produce new hair.30 Therefore, the bulge region constitutes a SC niche that makes multiple signals toward quiescence or proliferation stages.30–34 It is known that fibroblasts and adipocyte signals are able to inhibit the proliferation of HFSCs.34 Additionally, BMP6 and fibroblast growth factor 18 (FGF18) from bulge cells exert inhibitory effects on HFSC proliferation.34 Dihydrotestosterone (DHT) also inhibits HF growth.35 Agents that reduce DHT, such as Finasteride, promote hair regrowth by inhibiting Type II 5a-reductase.8,14,36 In contrast to these inhibitory effects, DPCs located at the base of the HF provide activation signals (Figure 1).18,34 The crosstalk between DPCs and HFSCs leads to inhibition of inhibitory effects with the resultant cell proliferation toward hair regeneration (anagen).30,31,37 With the self-renewal of HFSCs, the outer root sheath (ORS) forms, and signals from DPCs to the bulge cells diminish in a way that the bulge cells start again with their quiescent stage.4,34As mentioned earlier, Forkhead box C1 transcription factor has an important role in maintaining the threshold for HFSC activation.30 The knockdown of these factors in bulge cells reduces the cells’ threshold for proliferation, and the anagen cycle starts more frequently due to promotion of HFSC proliferation in shorter periods of time.30
Laser therapy
Light amplification by stimulated emission of radiation (LASER) generates electromagnetic radiation which is uniform in polarization, phase, and wavelength.45 Low-level laser therapy (LLLT), also called “cold laser” therapy, since it utilizes lower power densities than those needed to produce heating of tissue. Transdermal LLLT has been used for therapeutic purposes via photobiomodulation.46,47 Several clinical conditions, such as rheumatoid arthritis, mucositis, pain, and other inflammatory diseases, have been treated with these laser devices.48–50 LLLT promotes cell proliferation by stimulating cellular production of adenosine triphosphate and creating a shift in overall cell redox potential toward greater intracellular oxidation.51 The redox state of the cell regulates activation of signaling pathways that ultimately promotes high transcription factor activity and gene expression of factors associated with the cell cycle.52 Physical agents such as lasers have been also used to prevent hair loss in a wavelength range in the red and near infrared (600–1,070 nm).5,47,51,53 Laser therapy emits light that penetrates the scalp and promotes hair growth by increasing the blood flow.54 This increase gives rise to EC proliferation and migration due to upregulation of vascular endothelial growth factor (VEGF) and endothelial nitric oxide synthase.55,56 In addition, the laser energy itself stimulates metabolism in catagen or telogen follicles, resulting in the production of anagen hair.53,54A specific effect of LLLT has been demonstrated to promote proliferation of HFSCs, forcing the hair to start the anagen phase.57
Biologic agents that promote hair growth and their mechanisms of action
SC signaling
Recently, it has been found that SCs release factors that can promote hair growth.16 These factors and their mechanisms of action have been summarized in Table 3. These factors, known as “secretomes”, are able to promote skin regeneration, wound healing, and immunologic modulation, among other effects.58,59 Some of these factors, such as epidermal growth factor (EGF), basic fibroblast growth factor, hepatocyte growth factor (HGF) and HGF activator, VEGF, insulin-like growth factor (IGF), TGF-ß, and platelet-derived growth factor (PDGF), are able to provide signals that promote hair growth.15,60–64 As mentioned before, DPCs provide signals to HFSCs located in the bulge that proliferate and migrate either to the DP or to the epidermis to repopulate the basal layer (Figure 1).32,65 Enhancement in growth factor expression (except for EGF) has been reported when the adipose SCs are cultured in hypoxic conditions.15 Also, SCs increase their self-renewal capacity under these conditions.66–68 Low oxygen concentrations (1%–5%) increase the level of expression of SC factors that include VEGF, basic fibroblast growth factor, IGF binding protein 1 (IGFBP-1), IGF binding protein 2 (IGFBP-2), macrophage colony-stimulating factor (M-CSF), M-CSF receptor (M-CSFR), and PDGF receptor ß (PDGFR-ß).15,69,70 While these groups of factors promote HF growth in intact skin, another group of factors, such as M-CSF, M-CSFR, and interleukin-6, are involved in wound-induced hair neogenesis.71 HGF and HGF activator stimulate DPCs to promote proliferation of epithelial follicular cells.61 Epidermal growth factor promotes cellular migration via the activation of Wnt/ß-catenin signaling.60 VEGF promotes hair growth and increases the follicle size mainly by perifollicular angiogenesis.72 Blocking VEGF activity by neutralizing antibodies reduced the size and growth of the HF.72 PDGF and its receptor (PDGFR-a) are essential for follicular development by promoting upregulation of genes involved in HF differentiation and regulating the anagen phase in HFs.64,73 They are also expressed in neonatal skin cells that surround the HF.73 Monoclonal antibodies to PDGFR-a (APA5) produced failure in hair germ induction, supporting that PDGFR-a and its ligand have an essential role in hair differentiation and development.73 IGF-1 promotes proliferation, survival, and migration of HF cells.69,74 In addition, IGF binding proteins (IGFBPs) also promote hair growth and hair cell survival by regulating IGF-1 effects and its interaction with extracellular matrix proteins in the HF.70 Higher levels of IGF-1 and IGFBPs in beard DPCs suggest that IGF-1 levels are associated with androgens.74 Furthermore, DPCs from non-balding scalps showed significantly higher levels of IGF-1 and IGFBP-6, in contrast to DPCs from balding scalps.74
Table 3
Stem cell factors and small molecules that promote hair growth and their mechanisms of action
| Factor | Mechanism of action |
|---|---|
| HGF and HGF activator61 | Factor secreted by DPC that promotes proliferation of epithelial follicular cells |
| EGF60 | Promotes growth and migration of follicle ORS cells by activation of Wnt/ß-catenin signaling |
| bFGF62 | Promotes the development of hair follicle |
| IL-693 | Involved in WIHN through STAT3 activation |
| VEGF72 | Promotes perifollicular angiogenesis |
| TGF-ß63 | Stimulates the signaling pathways that regulate hair cycle |
| IGF-169 | Promotes proliferation, survival, and migration of hair follicle cells |
| IGFBP-1 to -670 | Regulates IGF-1 effects and its interaction with extracellular matrix proteins at the hair follicle level |
| BMP23 | Maintains DPC phenotype which is crucial for stimulation of hair follicle stem cell |
| BMPR1a23 | Maintains the proper identity of DPCs that is essential for specific DPC function |
| M-CSF71 | Involved in wound-induced hair regrowth |
| M-CSFR71 | Involved in wound-induced hair regrowth |
| PDGF and PDGFR-ß/-a64 | Upregulates the genes involved in hair follicle differentiation. Induction and regulation of anagen phase. PDGF and its receptors are essential for follicular development |
| Wnt3a97 | Involved in hair follicle development through ß-catenin signaling |
| PGE279,80 | Stimulates anagen phase in hair follicles |
| PGF2a and analogs79,80 | Promotes transition from telogen to anagen phase of the hair cycle |
| BIO98 | GSK-3 inhibitor |
| PGE2 or inhibition of PGD2 or PGD2 receptor D2/GPR4477 | Promotes follicle regeneration |
| Iron and l-lysine95 | Under investigation |
Abbreviations: bFGF, basic fibroblast growth factor; BIO, (2’Z,3’E)-6-bromoindirubin-3′-oxime; BMP, bone morphogenetic protein; DPCs, dermal papilla cells; EGF, epidermal growth factor; GSK-3, glycogen synthase kinase-3; HGF, hepatocyte growth factor; IGF-1, insulin-like growth factor 1; IGFBP-1, insulin-like growth factor-binding protein 1; IL-6, interleukin-6; M-CSF, microphage colony-stimulating factor; M-CSFR, microphage colony-stimulating factor receptor; ORS, outer root sheath; PDGF, platelet-derived growth factor; PDGFR-a, platelet-derived growth factor receptor alpha; PDGFR-ß, platelet-derived growth factor receptor beta; PGD2, prostaglandin D2; PGE2, prostaglandin E2; TGF-ß1, transforming growth factor ß1; VEGF, vascular endothelial growth factor; WIHN, wound-induced hair neogenesis; Wnt3a, wingless-type MMTV integration site family, member 3A.
Small molecules
Small molecules with low molecular weight (<900 Da) and the size of 10-9 m are organic compounds that are able to regulate some biologic processes.75 Some small molecules have been tested for their role in hair growth.76 Synthetic, non-peptidyl small molecules that act as agonists of the hedgehog pathway have the ability to promote follicular cycling in adult mouse skin.76 PGE2 and prostaglandin D2 (PGD2) have also been associated with the hair cycle (Table 3).77 PGD2 is elevated in the scalp of balding men and inhibits hair lengthening via GPR44 receptor.78 Also, it is known that PGE2 and PGF2a promote hair growth, while PGD2 inhibits this process.77,79 Prostaglandin analogs of PGF2a have been used originally to decrease ocular pressure in glaucoma with parallel effects in the growth of eyelashes, which suggests a specific effect in HF activation.80 PGD2 receptors are located in the upper and lower ORS region and in the DP, suggesting that these prostaglandins play an important role in hair cycle.81 Molecules such as quercetin are able to inhibit PGD2 and, in this way, promote hair growth.82–84 Antagonists of PGD2 receptor (formally named chemoattractant receptor-homologous expressed in Th2 cells) such as setipiprant have been used to treat allergic diseases such as asthma, but they also have beneficial effects in AGA.85–87 Another small molecule l-ascorbic acid 2-phosphate promotes proliferation of ORS keratinocytes through the secretion of IGF-1 from DPCs via phosphatidylinositol 3-kinase.88 Recently, it has been described that small-molecule inhibitors of Janus kinase–signal transducer and activator of transcription (JAK-STAT) pathway promote hair regrowth in humans.89 Janus kinase inhibitors are currently approved by the FDA for the treatment of some specific diseases such as psoriasis and other autoimmune-mediated diseases.90–94 Also, another group of small molecules such as iron and the amino acid l-Lysine are essential for hair growth (Table 3).95
Cellular therapy
The multipotent SCs in the bulge region of the HF receive signals from DPCs in order to proliferate and survive.27,28,65,84,96 It has been shown that Wnt/ß-catenin signaling is essential for the growth and maintenance of DPCs.19,97 These cells can be isolated and cultured in vitro with media supplemented with 10% fetal bovine serum and FGF-2.37,98 However, they lose versican expression that correlates with decrease in follicle-inducing activity in culture.98 Versican is the most abundant component of HF extracellular matrix.99 Inhibition of glycogen synthase kinase-3 by (2’Z,3’E)-6-bromoindirubin-3′-oxime (BIO) promotes hair growth in mouse vibrissa follicles in culture by activation of Wnt signaling.98 Therefore, the increase of Wnt signaling in DPCs apparently is one of the main factors that promote hair growth.19 DPCs have been also generated from human embryonic SCs that induced HF formation after murine transplantation.27
Platelet-rich plasma
Platelets are anucleate cells generated by fragmentation of megakaryocytes in the bone marrow.100 These cells are actively involved in the hemostatic process after releasing biologically active molecules (cytokines).100–102 Because of the platelets’ higher capacity to produce and release these factors, autologous platelet-rich plasma (PRP) has been used to treat chronic wounds.103 Therefore, PRP can be used as autologous therapy for regenerative purposes, for example, chondrogenic differentiation, wound healing, fat grafting, AGA, alopecia areata, facial scars, and dermal volume augmentation.101,104–108 PRP contains human platelets in a small volume that is five to seven times higher than in normal blood and it has been proven to be beneficial to treat AGA.10,105,109–111 The factors released by these platelets after their activation, such as PDGFs (PDGFaa, PDGFbb, PDGFab), TGF-ß1, TGF-ß2, EGF, VEGF, and FGF, promote proliferation of DPCs and, therefore, may be beneficial for AGA treatment.109,112–114 Clinical experiments indicate that patients with AGA treated with autologous PRP show improved hair count and thickness.109
In search of novel therapies
In this paper, we reviewed and discussed the use of therapeutic agents for hair regeneration and the knowledge to promote the development of new therapies for AGA based on the advances in regenerative medicine. The HF is a complex structure that grows when adequate signaling is provided to the HFSCs. These cells are located in the follicle bulge and receive signals from MSCs located in the dermis that are called DPCs. The secretory phenotype of DPCs is determined by local and circulatory signals or hormones. Recent discoveries have demonstrated that SCs in culture are able to activate DPCs and HFSCs and, in this way, promote hair growth. The study of these cellular signals can provide the necessary knowledge for developing more effective therapeutic agents for the treatment of AGA with minimal side effects. Therefore, advancements in the field of regenerative medicine may generate novel therapeutic alternatives. However, further research and clinical studies are needed to evaluate their efficacy.
Disclosure
The authors report no conflicts of interest in this work.
References
Blumeyer A, Tosti A, Messenger A, et al; European Dermatology Forum (EDF). Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Dtsch Dermatol Ges. 2011;9(Suppl 6):S1–S57. | ||
Ramos PM, Miot HA. Female pattern hair loss : a clinical and pathophysiological review. An Bras Dermatol. 2015;90(4):529–543. | ||
Otberg N, Finner AM, Shapiro J. Androgenetic alopecia. Endocrinolo Metab Clin North Am. 2007;36(2):379–398. | ||
Plikus MV, Chuong CM. Complex hair cycle domain patterns and regenerative hair waves in living rodents. J Invest Dermatol. 2008;128(5):1071–1080. | ||
McElwee KJ, Shapiro JS. Promising therapies for treating and/or preventing androgenic alopecia. Skin Therapy Lett. 2012;17(6):1–4. | ||
Perez-Mora N, Velasco C, Bermüdez F. Oral finasteride presents with sexual-unrelated withdrawal in long-term treated androgenic alopecia in men. Skinmed. 2015;13(3):179–183. | ||
Gupta AK, Charrette A. Topical minoxidil: systematic review and meta-analysis of its efficacy in androgenetic alopecia. Skinmed. 2015;13(3):185–189. | ||
Shapiro J, Kaufman KD. Use of finasteride in the treatment of men with androgenetic alopecia (male pattern hair loss). J Investig Dermatol Symp Proc. 2003;8(1):20–23. | ||
Rossi A, Anzalone A, Fortuna MC, et al. Multi-therapies in androgenetic alopecia: review and clinical experiences. Dermatol Ther. 2016;29(6):424–432. | ||
Varothai S, Bergfeld WF. Androgenetic alopecia: an evidence-based treatment update. Am J Clin Dermatol. 2014;15(3):217–230. | ||
Rossi A, Cantisani C, Melis L, Iorio A, Scali E, Calvieri S. Minoxidil use in dermatology, side effects and recent patents. Recent Pat Inflamm Allergy Drug Discov. 2012;6(2):130–136. | ||
Motofei IG, Rowland DL, Georgescu SR, Mircea T, Baleanu BC, Paunica S. Are hand preference and sexual orientation possible predicting factors for finasteride adverse effects in male androgenic alopecia? Exp Dermatol. 2016;25(7):557–558. | ||
Reijo Pera RA, Gleeson JG. Stems cells and regeneration: special review issue. Hum Mol Gen. 2008;17(R1):R1–R2. | ||
Jain R, De-Eknamkul W. Potential targets in the discovery of new hair growth promoters for androgenic alopecia. Expert Opin Ther Targets. 2014;18(7):787–806. | ||
Park BS, Kim WS, Choi JS, et al. Hair growth stimulated by conditioned medium of adipose-derived stem cells is enhanced by hypoxia : evidence of increased growth factor secretion. Biomed Res. 2010;31(1):27–34. | ||
Fukuoka H, Suga H. Hair regeneration treatment using adipose-derived stem cell conditioned medium :follow-up with trichograms. Eplasty. 2015;15:65–72. | ||
Du Y, Roh DS, Funderburgh ML, et al. Adipose-derived stem cells differentiate to keratocytes in vitro. Mol Vis. 2010;16:2680–2689. | ||
Zhang P, Kling RE, Ravuri SK, et al. A review of adipocyte lineage cells and dermal papilla cells in hair follicle regeneration. J Tissue Eng. 2014;5:2041731414556850. | ||
Tsai SY, Sennett R, Rezza A, et al. Wnt/ß-catenin signaling in dermal condensates is required for hair follicle formation. Dev Biol. 2014;385(2):179–188. | ||
Choi YS, Zhang Y, Xu M, et al. Distinct functions for Wnt/ß-catenin in hair follicle stem cell proliferation and survival and interfollicular epidermal homeostasis. Cell Stem Cell. 2013;13(6):720–733. | ||
Rao TP, Kuhl M. An updated overview on Wnt signaling pathways a prelude for more. Circ Res. 2010;106(12):1798–1806. | ||
Yano K, Brown LF, Detmar M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J Clin Invest. 2001;107(4):409–417. | ||
Rendl M, Polak L, Fuchs E. BMP signaling in dermal papilla cells is required for their hair follicle-inductive properties. Genes Dev. 2008;22(4):543–557. | ||
Talavera-Adame D, Gupta A, Kurtovic S, Chaiboonma KL, Arumugaswami V, Dafoe DC. Bone morphogenetic protein-2/-4 upregulation promoted by endothelial cells in coculture enhances mouse embryoid body differentiation. Stem Cells Dev. 2013;22(24):3252–3260. | ||
Talavera-Adame D, Wu G, He Y, et al. Endothelial Cells in Co-culture Enhance Embryonic Stem Cell Differentiation to Pancreatic Progenitors and Insulin-Producing Cells through BMP Signaling. Stem Cell Rev. 2011;7(3):532–543. | ||
Talavera-Adame D, Ng TT, Gupta A, Kurtovic S, Wu GD, Dafoe DC. Characterization of microvascular endothelial cells isolated from the dermis of adult mouse tails. Microvascular Res. 2011;82(2):97–104. | ||
Gnedeva K, Vorotelyak E, Cimadamore F, et al. Derivation of hair-inducing cell from human pluripotent stem cells. PLoS One. 2015;10(1):1–14. | ||
Lavker RM, Sun T, Oshima H, et al. Hair follicle stem cells. J Investig Dermatol Symp Proc. 2003;8(1):28–38. | ||
Bernard B. Advances in understanding hair growth. F1000Res. 2016;5:1–8. | ||
Lay K, Kume T, Fuchs E. FOXC1 maintains the hair follicle stem cell niche and governs stem cell quiescence to preserve long-term tissue-regenerating potential. Proc Natl Acad Sci U S A. 2016;113(1): E1506–E1515. | ||
Leirós GJ, Attorresi AI, Balañá ME. Hair follicle stem cell differentiation is inhibited through cross-talk between Wnt/ß-catenin and androgen signalling in dermal papilla cells from patients with androgenetic alopecia. Br J Dermatol. 2012;166(5):1035–1042. | ||
Chacon-Martinez CA, Klose M, Niemann C, Glauche I, Wickström SA. Hair follicle stem cells= cultures reveal self-organizing plasticity of stem cells and their progeny. EMBO J. 2017;36(2):151–164. | ||
Soler AP, Gilliard G, Megosh LC, O’Brien TG. Modulation of murine hair follicle function by alterations in ornithine decarboxylase activity. J Invest Dermatol. 1996;106(5):1108–1113. | ||
Hsu YC, Pasolli HA, Fuchs E. Dynamics between stem cells, nich and progeny in the hair follicle. Cell. 2011;144(1):92–105. | ||
Kang JI, Kim SC, Kim MK, et al. Effects of dihydrotestosterone on rat dermal papilla cells in vitro. Eur J Pharmacol. 2015;757:74–83. | ||
Yamana K, Labrie F, Luu-The V. Human type 3 5a-reductase is expressed in peripheral tissues at higher levels than types 1 and 2 and its activity is potently inhibited by finasteride and dutasteride. Horm Mol Biol Clin Investig. 2010;2(3):293–299. | ||
Osada A, Iwabuchi T, Kishimoto J, Hamazaki TS, Okochi H. Long-term culture of mouse vibrissal dermal papilla cells and de novo hair follicle induction. Tissue Eng. 2007;13(5):975–982. | ||
Choi GS, Kim JH, Oh SY, et al. Safety and tolerability of the dual 5-alpha reductase inhibitor dutasteride in the treatment of androgenetic alopecia. Ann Dermatol. 2016;28(4):444–450. | ||
Carson C 3rd, Rittmaster R. The role of dihydrotestosterone in benign prostatic hyperplasia. Urology. 2003;61(4 Suppl 1):2–7. | ||
Kamimura A, Takahashi T. Procyanidin B-2, extracted from apples, promotes hair growth: a laboratory study. Br J Dermatol. 2002;146(1):41–51. | ||
Kamimura A, Takahashi T. Procyanidin B-3, isolated from barley and identified as a hair-growth stimulant, has the potential to counteract inhibitory regulation by TGF-beta1. Exp Dermatol. 2002;11(6):532–541. | ||
Ulbricht C, Basch E, Bent S, et al. Evidence-based systematic review of saw palmetto by the Natural Standard Research Collaboration. J Soc Integr Oncol. 2006;4(4):170–186. | ||
Rondanelli M, Perna S, Peroni G, Guido D. A bibliometric study of scientific literature in Scopus on botanicals for treatment of androgenetic alopecia. J Cosmet Dermatol. 2015;15(2):120–130. | ||
Blume-Peytavi U, Kunte C, Krisp A, Garcia Bartels N, Ellwanger U, Hoffmann R. [Comparison of the efficacy and safety of topical minoxidil and topical alfatradiol in the treatment of androgenetic alopecia in women.] J Dtsch Dermatol Ges. 2007;5(5):391–395. German. | ||
Farivar S, Malekshahabi T, Shiari R. Biological effects of low level laser therapy. J Lasers Med Sci. 2014;5(2):58–62. | ||
Maiman TH. Biomedical lasers evolve toward clinical applications. Hosp Manage. 1966;101(4):39–41. | ||
Cung H, Dai T, Sharma SK, et al. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2013;40(2):516–533. | ||
Bjordal JM, Couppé C, Chow RT, Tunér J, Ljunggren EA. A systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders. The Aust J Physiother. 2003;49(2):107–116. | ||
Brosseau L, Welch V, Wells G, et al. Low level laser therapy (classes I, II and III) in the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. 2005;19(2):CD002049. | ||
Cauwels RGEC, Martens LC. Low level laser therapy in oral mucositis: a pilot study. Eur Arch Paediatr Dent. 2011;12(2):118–123. | ||
Schindl A, Schindl M, Pernerstorfer-Schön H, Schindl L. Low-intensity laser therapy: a review. J Investig Med. 2000;48(5):312–326. | ||
Liu H, Colavitti R, Rovira II, Finkel T. Redox-dependent transcriptional regulation. Cir Res. 2005;97(10):967–974. | ||
Gupta AK, Lyons DCA, Abramovits W. Low-level laser/light therapy for androgenetic alopecia. Skinmed. 2014;12(3):145–147. | ||
Jimenez JJ, Wikramanayake TC, Bergfeld W, et al. Efficacy and safety of a low-level laser device in the treatment of male and female pattern hair loss: a multicenter, randomized, sham device-controlled, double-blind study. Am J Clin Dermat. 2014;15(2):115–127. | ||
Chen CH, Hung HS, Hsu SH. Low-energy laser irradiation increases endothelial cell proliferation, migration, and eNOS gene expression possibly via PI3K signal pathway. Lasers Surg Med. 2008;40(1):46–54. | ||
Tuby H, Maltz L, Oron U. Modulations of VEGF and iNOS in the rat heart by low level laser therapy are associated with cardioprotection and enhanced angiogenesis. Lasers Surg Med. 2006;38(7):682–688. | ||
Avci P, Gupta GK, Clark J, Wikonkal N, Hamblin MR. Low-level laser (light) therapy (LLLT) for treatment of hair loss. Laser Surg Med. 2015;46(2):144–151. | ||
Rodrigues C, de Assis AM, Moura DJ, et al. New therapy of skin repair combining adipose-derived mesenchymal stem cells with sodium carboxymethylcellulose scaffold in a pre-clinical rat model. PloS One. 2014;9(5):e96241. | ||
Gimble JM, Katz AJ, Bunnell BA. Adipose-derived stem cells for regenerative medicine. Cir Res. 2007;100(9):1249–1260. | ||
Zhang H, Nan W, Wang S, et al. Epidermal growth factor promotes proliferation and migration of follicular outer root sheath cells via Wnt/ß-catenin signaling. Cell Physiol Biochem. 2016;39(1):360–370. | ||
Lee YR, Yamazaki M, Mitsui S, Tsuboi R, Ogawa H. Hepatocyte growth factor (HGF) activator expressed in hair follicles is involved in in vitro HGF-dependent hair follicle elongation. J Dermatol Sci. 2001;25(2):156–163. | ||
du Cros DL. Fibroblast growth factor influences the development and cycling of murine hair follicles. Dev Biol. 1993;156(2):444–453. | ||
Niimori D, Kawano R, Felemban A, et al. Tsukushi controls the hair cycle by regulating TGF-ß1 signaling. Dev Biol. 2012;372(1):81–87. | ||
Tomita Y, Akiyama M, Shimizu H. PDGF isoforms induce and maintain anagen phase of murine hair follicles. J Dermatol Sci. 2006;43(2):105–115. | ||
Ohyama M, Terunuma A, Tock CL, et al. Characterization and isolation of stem cell – enriched human hair follicle bulge cells. J Clin Invest. 2006;116(1):249–260. | ||
Grayson WL, Zhao F, Bunnell B, Ma T. Hypoxia enhances proliferation and tissue formation of human mesenchymal stem cells. Biochem Biophys Res Commun. 2007;358(3):948–953. | ||
Potier E, Ferreira E, Andriamanalijaona R, et al. Hypoxia affects mesenchymal stromal cell osteogenic differentiation and angiogenic factor expression. Bone. 2007;40(4):1078–1087. | ||
Ren H, Cao Y, Zhao Q, et al. Proliferation and differentiation of bone marrow stromal cells under hypoxic conditions. Biochem Biophys Res Commun. 2006;347(1):12–21. | ||
Su HY, Hickford JG, Bickerstaffe R, Palmer BR. Insulin-like growth factor 1 and hair growth. Dermatol Online J. 1999;5(2):1. | ||
Batch JA, Mercuri FA, Werther GA. Identification and localization of insulin-like growth factor-binding protein (IGFBP) messenger RNAs in human hair follicle dermal papilla. J Invest Dermatol. 1996;106(3):471–475. | ||
Osaka N, Takahashi T, Murakami S, et al. ASK1-dependent recruitment and activation of macrophages induce hair growth in skin wounds. J Cell Biol. 2007;176(7):903–909. | ||
Yano K, Brown LF, Detmar M. Control of hair growth and follicle size by VEGF-mediated angiogenesis. J Clin Invest. 2001;107(4):409–417. | ||
Takakura N, Yoshida H, Kunisada T, Nishikawa S, Nishikawa SI. Involvement of platelet-derived growth factor receptor-a in hair canal formation. J Invest Dermatol. 1996;107(5):770–777. | ||
Panchaprateep R, Asawanonda P. Insulin-like growth factor-1: roles in androgenetic alopecia. Exp Dermatol. 2014;23(3):216–218. | ||
Castoreno AB, Eggert US. Small molecule probes of cellular pathways and networks. ACS Chem Biol. 2011;6(1):86–94. | ||
Paladini RD, Saleh J, Qian C, Xu GX, Rubin LL. Modulation of hair growth with small molecule agonists of the hedgehog signaling pathway. J Iinvest Dermatol. 2005;125(4):638–646. | ||
Nieves A, Garza LA. Does prostaglandin D2 hold the cure to male pattern baldness? Exp Dematol. 2014;(29):224–227. | ||
Nelson AM, Loy DE, Lawson JA, Katseff AS, Fitzgerald GA, Garza LA. Prostaglandin D2 inhibits wound-induced hair follicle neogenesis through the receptor Gpr44. J Invest Dermatol. 2013;133(4):881–889. | ||
Sasaki S, Hozumi Y, Kondo S. Influence of prostaglandin F2alpha and its analogues on hair regrowth and follicular melanogenesis in a murine model. Exp Dermatol. 2005;14(5):323–328. | ||
Choi YM, Diehl J, Levins PC. Promising alternative clinical uses of prostaglandin F2a analogs: beyond the eyelashes. J Am Acad Dermatol. 2015;72(4):712–716. | ||
Colombe L, Michelet JF, Bernard BA. Prostanoid receptors in anagen human hair follicles. Exp Dermatol. 2008;17(1):63–72. | ||
Zhang Q, Major MB, Takanashi S, et al. Small-molecule synergist of the Wnt/beta-catenin signaling pathway. Proc Natl Acad Sci U S A. 2007;104(18):7444–7448. | ||
Fong P, Tong HH, Ng KH, Lao CK, Chong CI, Chao CM. In silicoprediction of prostaglandin D2 synthase inhibitors from herbal constituents for the treatment of hair loss. J Ethnopharmacol. 2015;175:470–480. | ||
Weng Z, Zhang B, Asadi S, et al. Quercetin is more effective than cromolyn in blocking human mast cell cytokine release and inhibits contact dermatitis and photosensitivity in humans. PloS One. 2012;7(3):e33805. | ||
Norman P. Update on the status of DP2 receptor antagonists; from proof of concept through clinical failures to promising new drugs. Expert Opin Investig Drugs. 2014;23(1):55–66. | ||
Pettipher R. The roles of the prostaglandin D(2) receptors DP(1) and CRTH2 in promoting allergic responses. Br J Pharmacol. 2008;153(Suppl 1):S191–S199. | ||
Garza LA, Liu Y, Yang Z, et al. Prostaglandin D2 inhibits hair growth and is elevated in bald scalp of men with androgenetic alopecia. Sci Transl Med. 2012;4(126):126ra34. | ||
Kwack MH, Shin SH, Kim SR, et al. I-Ascorbic acid 2-phosphate promotes elongation of hair shafts via the secretion of insulin-like growth factor-1 from dermal papilla cells through phosphatidylinositol 3-kinase. Br J Dermatol. 2009;160(6):1157–1162. | ||
Harel S, Higgins CA, Cerise JE, et al. Pharmacologic inhibition of JAK-STAT signaling promotes hair growth. Sci Adv. 2015;1(9):e1500973. | ||
Quintás-cardama A, Vaddi K, Liu P, et al. INCB018424 : therapeutic implications for the treatment of myeloproliferative neoplasms Preclinical characterization of the selective JAK1 / 2 inhibitor INCB018424 : therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2014;115(15):3109–3117. | ||
Geyer HL, Mesa RA. Therapy for myeloproliferative neoplasms: when, which agent, and how? Hematology Am Soc Hematol Educ Program. 2014;2014(1):277–286. | ||
Ghoreschi K, Jesson MI, Li X, et al. Modulation of innate and adaptive immune responses by tofacitinib (CP-690,550). J Immunol. 2012;186(7):4234–4243. | ||
Kontzias A, Laurence A, Gadina M, O’Shea JJ. Kinase inhibitors in the treatment of immune-mediated disease. F1000 Med Rep. 2012;4:5. | ||
Bao L, Zhang H, Chan LS. The involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitis. JAKSTAT. 2013;2(3):1–8. | ||
Rushton DH. Nutritional factors and hair loss. Clin Exp Dermatol. 2002;27(5):396–404. | ||
Oshima H, Rochat A, Kedzia C, Kobayashi K, Barrandon Y. Morphogenesis and renewal of hair follicles from adult multipotent stem cells. Cell. 2001;104(2):233–245. | ||
Huelsken J, Vogel R, Erdmann B, Cotsarelis G, Birchmeier W. beta-Catenin controls hair follicle morphogenesis and stem cell differentiation in the skin. Cell. 2001;105(4):533–545. | ||
Yamauchi K, Kurosaka A. Inhibition of glycogen synthase kinase-3 enhances the expression of alkaline phosphatase and insulin-like growth factor-1 in human primary dermal papilla cell culture and maintains mouse hair bulbs in organ culture. Arch Dermatol Res. 2009;301(5):357–365. | ||
Sotoodehnejadnematalahi F, Burke B. Structure, function and regulation of versican: the most abundant type of proteoglycan in the extracellular matrix. Acta Med Iran. 2013;51(11):740–750. | ||
Xu XR, Zhang D, Oswald BE, et al. Platelets are versatile cells: new discoveries in hemostasis, thrombosis, immune responses, tumor metastasis and beyond. Crit Rev Clin Lab Sci. 2016;53(6):409–430. | ||
Lacci KM, Dardik A. Platelet-rich plasma: support for its use in wound healing. Yale J Biol Med. 2010;83(1):1–9. | ||
Mussano F, Genova T, Munaron L, Petrillo S, Erovigni F, Carossa S. Cytokine, chemokine, and growth factor profile of platelet-rich plasma. Platelets. 2016;27(5):467–471. | ||
Martinez-Zapata MJ, Martí-Carvajal AJ, Solà I, et al. Autologous platelet-rich plasma for treating chronic wounds. Cochrane Database Syst Rev. 2016;(5):CD006899. | ||
Modarressi A. Platlet Rich Plasma (PRP) improves fat grafting outcomes. World J Plast Surg. 2013;2(1):6–13. | ||
Gentile P, Garcovich S, Bielli A, Scioli MG, Orlandi A, Cervelli V. The Effect of platelet-rich plasma in hair regrowth: a randomized placebo-controlled trial. Stem Cells Transl Med. 2015;4(11):1317–1323. | ||
Lynch MD, Bashir S. Applications of platelet-rich plasma in dermatology: a critical appraisal of the literature. J Dermatolog Treat. 2016;27(3):285–289. | ||
Trink A, Sorbellini E, Bezzola P, et al. A randomized, double-blind, placebo- and active-controlled, half-head study to evaluate the effects of platelet-rich plasma on alopecia areata. Br J Dermatol. 2013;169(3):690–694. | ||
Oh Y, Kim BJ, Kim MN. Depressed facial scars successfully treated with autologous platelet-rich plasma and light-emitting diode phototherapy at 830 nm. Ann Dermatol. 2014;26(3):417–418. | ||
Singhal P, Agarwal S, Dhot PS, Sayal SK. Efficacy of platelet-rich plasma in treatment of androgenic alopecia. Asian J Transfus Sci. 2015;9(2):159–162. | ||
Valente Duarte de Sousa IC, Tosti A. New investigational drugs for androgenetic alopecia. Expert Opin Investig Drugs. 2013;22(5):573–589. | ||
Alves R, Grimalt R. Randomized placebo-controlled, double-blind, half-head study to assess the efficacy of platelet-rich plasma on the treatment of androgenetic alopecia. Dermatol Surg. 2016;42(4):491–497. | ||
Cho JW, Kim SA, Lee KS. Platelet-rich plasma induces increased expression of G1 cell cycle regulators, type I collagen, and matrix metalloproteinase-1 in human skin fibroblasts. Int J Mol Med. 2012;29(1):32–36. | ||
Mehta V. Platelet-rich plasma: a review of the science and possible clinical applications. Orthopedics. 2010;33(2):111. | ||
Leo MS, Kumar AS, Kirit R, Konathan R, Sivamani RK. Systematic review of the use of platelet-rich plasma in aesthetic dermatology. J Cosmet Dermatol. 2015;14(4):315–323. |
- Published in Blog
What’s all the fuss about Regenerative Medicine?

In popular media, the term Regenerative Medicine, or Stem Cell Therapy, are becoming buzz words. This is because the field of medicine and healthcare is expanding and advancing every day, and many new treatments for otherwise common ailments are being discovered. These conditions range from burns, joint pain, strain, and pretty much every other common ailment out there.
Many patients have given up hope with trying to find traditional medicines that work. This is why many people are flocking to try Regenerative Medicine. This is also something that many people who are into holistic healing are trying, as it is simply the body working to heal itself.
Regenerative Medicine works as it takes a sample of your own blood, bone marrow, and other tissues, and then it goes through a process in which to take out a certain material known as Platelet-Rich Plasma. This PRP is then applied to the infected area, so that your body’s own platelets can work to heal your body back to full health, without having to worry about any invasive surgeries.
A good question to ask is why our body does this do this itself. Well, this is because research has shown that by isolating them, they activate, and as a result when injected back into the body start to work harder to fix the issues, such as in a joint, or helping to relieve pain. Many patients who try it say they have gotten good results from the treatment.

Many doctors predict that this therapy will help physicians provide a more non-intrusive treatment that has fewer side effects, and can be big within the coming years. Many compare it to the invention of penicillin with how important it is. It is even growing in popularity with many physicians using training courses to help their patients, leaving many of them happier and healthier.
- Published in Blog
7 PRP Treatments That Are Popular Right Now

The time it takes to draw a patient’s blood, add a little citrate, and use a centrifugal machine with a PRP kit is only 15-20 minutes. This is the amount of time needed to create Platelet-Rich Plasma, or PRP. This can then be used for many purposes, using speeding up a patients recovery.
PRP is by far the best healing agent that has growth factors and platelets to help with the healing process, which is also completely free and natural to obtain.
What are The Advantages Of Using PRP Correctly?
It is easy to create PRP simpy by placing blood in a centrifuge, but it can have very little, if any, platelets, and would otherwise be useless. However, with the right equipment, you can make PRP with up to 7x the amount of platelets. This can be amplified by using fat tissue and collagen fibers to create a PRP matrix.
7 Popular PRP Treatments
- Facial Treatments
Many skin centers are thriving due to being one of the first to adopt PRP therapies. With the lack of side effects or down time, it became incredibly popular. These treatments include wrinkle reduction, skin rejuvenation, dark circle and bag erasure, rosacea treatment, and even lip augmentation.
One popular and generic treatment option includes combining PRP and a treatment known as microneedling. When this is applied, it’s effects are similar to Botox, or facelifts, for far less cost and side effects.
- Hair Loss
PRP growth factors can be beneficial when it comes to reversing non-genetic early stage hair loss. Despite there being a huge market for this, almost no practitioners actually utilize it. Many clients have seen promise after hair thinning, and many have seen beard regrowth over time.
- Arthritis and Cartilage
Arthritis treatments alone cost patients 6.4 billion dollars in 2013 for the US alone, with projections of up to 9 billion by the end of the decade. However, unlike the other treatments, PRP is seen as the only treatment that can not just reduce symptoms, but also regrow the cartilage. One of the most popular examples would be treatments for Temporomandibulaar Joint Osteoarthritis.
- Anti-aging Properties
When it comes to the anti-aging market, there are a endless number of treatments and procures available. Yet, none of them even stand close to the effectiveness of PRP therapy. PRP combined with Microneedling can ve highly effective for strech marks, acne scars, breast augmentation, and even skin conditions like Lichen Sclerosus.
- Pain Relief and Musculoskeletal Healing
There are a ton of treatments in this category, with many of them being incredibly more effective than leading treatments. These include healing Rotator Cuffs, Tennis Elbow, Achilles Tendonitis, Patellar Tendonitis, Back Pain, Hip and Pelvic problems, Degenerative Disc Disease, Golfer’s Elbow, Labaral Tear, Brusitis, neck pain, avascular Necrosis, and even pain related to nerve regeneration.
Almost all of these treatment, as opposed to those in other categories on this list, also use ultrasound guidance when injecting the PRP directly into the affected tissue. This can allow patients to see fantastic results in as little as 2 weeks.
- Fertility
Ovarian Rejuvination is where PRP is injected directly into a woman’s ovaries. This is meant to help reverse menopause and help lower fertility issues. This treatment can even be used for sexual regeneration. Although similar, this treatment is not the same as other treatments where PRO is injected into the vagina, and is supposed to treat looseness, dryness, low sex drive, and incontinence.
- COPD (Chronic Obstructive Pulmonary Disease)
Allergies, asthma, and COPD are among the growing list of things that PRP is being used as a treatment for. For this to work, the PRP is mixed with a saline solution, and then, using a nebulizer, is inhaled, and helps to regenerate the lung tissue.
Although it can take up to 2 months for patients to see the effects, many are seeing improvements. Almost 1 million people suffer from COPD a year, so anything that can help treat the condition is beneficial.
The Future
PRP has been trending rather well in the recent years, and seems to be here for the long term. Not only it is a fully natural remedy, but it is one that works better than most or all traditional treatments. Many like it due to the fact that there are few side effects, it only takes a short amount of time, and there is no recovery period.
PRP has been adopted by thousands of clinics and practices throughout the US and the world. The demand for these treatments have been increasing almost faster than practices are choosing to provide them. Many patients are even willing to travel long distances just to receive these treatments.
So are you providing PRP treatments yet?

- Published in Blog
Stem Cell Platelet-Rich Plasma: The Best Regenerative Therapy?

To understand why stem cell platelet-rich plasma or co-transplantation of Adipose-derived mesenchymal stem cells and PRP, is such a remarkable idea in regenerative medicine, let’s spend a little time looking at the mechanics of PRP.
Platelet-Rich Plasma’s Role As Repairmen
The one thing that makes Platelet-Rich Plasma a hero in several fields (if not all) of medicine is the fact that the diverse growth factors in it are able to stimulate stem cell proliferation and cell differentiation (the factors that determine effective tissue regeneration and healing) on any part of the body.
These growth factors are abundant in the blood and act as the natural repairmen of tissues.
In the perfect scenario, there’s plenty of blood flow to every part of the body and these “repairmen” are always on-call to address any healing needs that may arise. However, if the injured area has a poor blood supply — especially areas that are constantly move like tendons, ligaments and joints — demand for these repairmen can outgrow supply. Meaning, healing (or regeneration of tissues) is put on hold till further repairmen are available.
The train of Platelet-Rich Plasma then arrives with enough of these repairmen to warrant resumption of healing.
There’s another part of this picture we haven’t talked about so far: stem cells.
As far as Platelet-Rich Plasma and it’s growth factors are concerned, they are mere repairmen. They can’t do the work by themselves. They need the basic raw materials to work with. And that raw material here is the stem cells.
Stem cells are the ones actually being regenerated to form new tissues for healing.
Stem Cells As The Raw Materials For PRP
Stem cells are the only raw materials that PRP works with for regeneration. These are like the fundamental building blocks of all other cells. These cells can be can be guided into becoming specialized cells under the right conditions.
In addition, they can also divide themselves to form new stem cells or new specialized cells.
So for Platelet-Rich Plasma to work well, it needs to be applied to an area with lots of stem cells like the heart, liver, blood vessels etc. Incidentally Platelet-Rich Plasma’s healing properties were first discovered by cardiac surgeons who played with concentrated blood for faster healing of heart after surgery and it showed tremendous promise because stem cells are abundant in heart tissues.
But what if healing is needed in an area where there are not much stem cells?
With the new developments in stem cell technology that can be solved too. Because now we can supply the stem cells to areas where there are less like the joints, ligaments and tendons. For this, scientists usually use “mesenchymal stem cell” or MSCs. These are cells isolated from stroma and can differentiate to form adipocytes, cartilage, bone, tendons, muscle, and skin.
The most easiest way is to harvest it from adipose tissue or fat that we call Adipose-derived mesenchymal stem cells or ADSC.
Stem Cell Platelet-Rich Plasma
Supplying Both PRP And Stem Cells For Regeneration
In regions with hypoxia (poor blood supply) like joints, meniscus tissue, rotator cuff, spinal discs etc the supply of platelets (and therefore growth factors) as well as the stem cells are limited. So what if we supplied both the stem cells and Platelet-Rich Plasma for triggering the regeneration process?
That’s the question these Japanese scientists answered in their research. Here’s another group of scientists who took on the same challenge.
They used Adipose-derived mesenchymal stem cells (ADSC) which is known for their ease of isolation and extensive differentiation potential. These researchers noted that these stem cells often can’t survive in areas of local hypoxia, oxidative stress and inflammation – thereby making them ineffective. However, when Platelet-Rich Plasma (or thrombin-activated PRP) is added to ADSC, it kept them alive for prolonged periods and the growth factors in the Platelet-Rich Plasma triggered cell differentiation and proliferation more easily.
Why This Exact Combination Is The Future
Done this way, both Adipose-derived mesenchymal stem cells (ADSC) and Platelet-Rich Plasma are raw materials for healing that’s already available in plenty in almost every one (there are exceptions of course). That means, for complete healing to take place this combination treatment, still in it’s very primitive stage of development, may have the potential to replace expensive synthetic drugs that carry complex unexplained side effects. The procedure takes our body’s natural healing agents — stem cells from body fat and PRP from blood — and then inject it inside knee or other joints (or other areas where they are insufficient) for regeneration.
Isn’t that like the most wonderful thing ever?
Whether it’s cartilage cell, or a bone cell, or a collagen cell for ligaments and tendons that needs to be healed, all you need is a same-day procedure by a local, but specialized doctor, using the natural ingredients of the body.
I believe this special combo is a huge win for Platelet-Rich Plasma.
The Challenges For Growing Adoption Of This Treatment
We know Platelet-Rich Plasma has safe, yet high-speed recovery potential with it’s multiple growth factors. And it is effective in regenerative healing of cartilage injuries – the most toughest injuries to heal – as well as Osteoarthritis. However the challenges are Platelet Quality. We need to somehow ensure the Platelet-Rich Plasma quality is uniform. Currently it varies from two to several fold above baseline concentration based on donor’s physical condition.
Next we need to identify the exact PRP growth factors that promote ADSC proliferation. Scientists believe growth factors such as basic fibroblast growth factor (bFGF), epidermal growth factor, and platelet-derived growth factor stimulate stem cell proliferation while some growth factors under certain conditions are known to inhibit the process.
The percentage of PRP matters too. 5 percent, 10 percent, 15 percent and 20 percent Platelet-Rich Plasma in ADSC are tested by scientists.
The Only Treatment In Modern Medicine For Cartilage Regeneration
The bottom line is that Stem Cell Platelet-Rich Plasma or ADSC + PRP procedure is the only treatment in modern medicine that has showed cartilage regeneration. So it’s too important to ignore. And it could one of greatest advances that science has brought to the millions of people suffering from serious pain in their joints, knee and spine as well people suffering from all kinds of tendon diseases and injuries.
- Published in Blog
