New Stem Cell Research Shows Promising Results for Muscular Dystrophy

The term muscular dystrophy (MD) refers to a group of disorders in which a genetic abnormality causes muscles responsible for controlling movement to become weak, and muscle mass to be lost. These inherited disorders usually affect voluntary (skeletal) muscles, although weakness can also extend to the muscles that control respiration and swallowing.
Given that the genetic mutations triggering MD interfere with the normal production of certain critical proteins, the body is not able to reverse muscle weakening or loss of mass, so even when the disease progresses slowly, it eventually affects one’s ability to walk in a more or less conducive manner.
Who is affected by muscular dystrophy?
In most cases MD appears in infancy, but it’s not uncommon for symptoms to start manifesting in teens or adults.
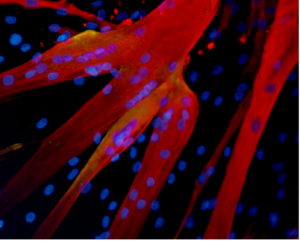
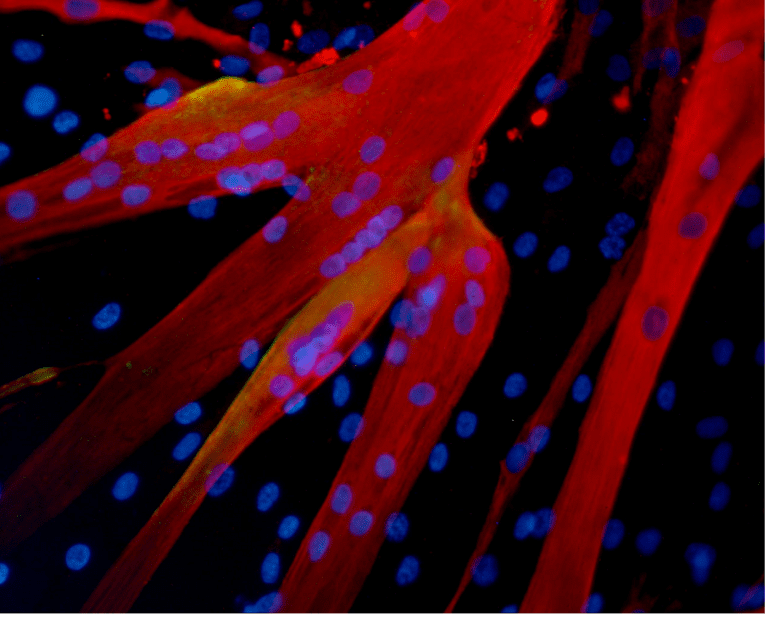
Muscle fibers formed in the lab by human mesoangioblasts (image: eurostemcell).
Although the manifestations are similar, their severity varies depending on the age at which the disease occurs. In some, the symptoms are mild and sufferers are able to continue living almost normally, while in others the ailment is extremely disabling and can lead to muscle wasting, loss of the ability to walk, and even death.
There are different kinds of muscular dystrophy, the most common and severe form being Duchenne muscular dystrophy (DMD) Caused by a genetic flaw or defect, Duchenne MD is more common in males than females [1} and affects about 1 in every 3,500 boys worldwide.
The onset of Duchenne muscular dystrophy occurs between the ages of 2 and 6, and evolves slowly. Muscles becoming weaker year after year, and the spine and limbs becoming progressively deformed. In most cases, children affected by this form of the disease become wheelchair dependent by the age of 12.
People suffering from Duchenne MD often die in their 20s, and those who survive usually experience some degree of cognitive impairment. The shortening of tendons and muscles limits the mobility of sufferers even more, and breathing and heart problems can occur.
Treatments for Duchenne muscular dystrophy
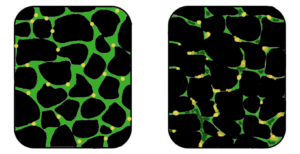
Muscular dystrophy is a genetic disorder where the muscle tissue wastes away and loses function. In the affected muscle (left), the tissue has become disorganized and the concentration of dystrophin (green), an important protein in normal muscle functioning, is greatly reduced. (Image: Wikipedia)
There is currently no known cure for DMD, but there are treatments that help to reduce some of the symptoms and strengthen the patient’s muscles to some degree.
Physiotherapy is commonly used for slowing down the loss of muscle mass and for maintaining flexibility or reducing muscle stiffness. Steroids are also used to slow down muscle wasting, but the severe side effects of steroids often cause more harm than good, such as bone weakening or cardiovascular problems.
In a healthy organism, damaged muscles repair themselves thanks to a series of cells that include muscle stem cells, called satellite cells. In Duchene muscular dystrophy, the muscles lack dystrophin, the protein needed for maintaining the integrity of muscle fibers. Without this protein, the burden placed on the body’s naturally occurring muscle stem cells is too intense, rendering the cells unable to repair damaged muscle tissue or to generate new muscle mass to replace wasted mass [6].
For this reason, scar tissue and fat cells take the place of damaged muscle tissue, contributing to muscle weakening and, over time, cause muscles to lose their functional ability. Would it be possible for the damaged muscle fibers to regain their regenerative ability with help from transplanted stem cells?
Research suggests stem cells could be a potential solution for muscle wasting

(Click on image to enlarge) Considerable efforts are underway to develop drugs and biologics (cell and gene therapy) to address the primary problem in Duchenne—the absence of dystrophin. Restoring dystrophin or replacing dystrophin with replacement protein are considered foundational therapies.
Different strategies involving stem cells for muscular dystrophy may be on the horizon, research suggests. Scientists have been using stem cells isolated from muscle tissue, bone marrow and blood vessels in lab animals to regenerate muscle fibers that are deficient in dystrophin[3] and results are encouraging.
In 2006, researchers managed to restore mobility in two afflicted dogs using stem cells isolated from muscle blood vessels [4], and in 2007 scientists managed to treat Duchenne MD in research mice using a combination of genetic correction and stem cells [3]. The latter study showed that it is possible to correct the genetic error in the cells that no longer produce dystrophin protein, and inject corrected cells stimulating the regeneration of muscles.
Researchers at the Harvard Stem Cell Institute obtained similar results, demonstrating that transplanted muscle stem cells can improve function in mice with MD, while replenishing the stem cell population in muscle fibers [5].
Although it’s still too early to say whether stem cells can cure DMD in humans, it’s clear that there are some promising stem-cell-based approaches for Duchenne MD. One solution is to replace the defective stem cells with healthy stem cells, as these may be able to generate working muscle fibers to replace damaged muscle fibers .
A second solution would be to reduce the inflammation that speeds up the loss and weakening of muscles using certain types of stem cells [2]. Combined treatments, such as mixing stem cell therapies with gene therapies are also being tested and may prove successful in the near future.
References:
- http://www.mayoclinic.org/diseases-conditions/muscular-dystrophy/basics/definition/con-20021240
- http://www.eurostemcell.org/factsheet/muscular-dystrophy-how-could-stem-cells-help
- https://www.mda.org/disease/duchenne-muscular-dystrophy/research
- http://quest.mda.org/article/scientists-bullish-stem-cells-muscle-repair
- http://hsci.harvard.edu/stem-cells-used-treat-muscular-dystrophy-mice
- https://med.stanford.edu/news/all-news/2014/12/stem-cells-faulty-in-duchenne-muscular-dystrophy.html
- Published in Blog
Scientists Confirm Reprogrammed Adult Stem Cells Identical to Embryonic Stem Cells

Photo: iPS cells feature – reprogrammed stem cells: Credit: Moscow Institute of Physics and Technology
Russian researchers have concluded that reprogramming does not create differences between reprogrammed and embryonic stem cells.
Stem cells are specialized, undifferentiated cells that can divide and have the remarkable potential to develop into many different cell types in the body during early life and growth. They serve as a sort of internal repair system in many tissues, dividing essentially without limit to replenish other cells. When a stem cell divides, each new cell has the potential either to remain a stem cell or become another more specialized cell type, such as a muscle cell, a red blood cell, or a brain cell. Scientists
distinguish several types of stem cells—pluripotent stem cells can potentially produce any cell in the body. No pluripotent stem cells exist in an adult body, rather they are found naturally in
early embryos.
There are two ways to harvest pluripotent stem cells. The first is to extract them from the excess embryos produced during invitro fertilization procedures, although this practice is still ethically and technically controversial because it does destroy an embryo that could have been implanted. For this reason, researchers came up with the second way to get pluripotent stem cells— reprogramming adult cells.
Reprogramming, the process of “turning on” genes that are active in a stem cell and “turning off” genes that are responsible for cell specialization was pioneered by Shinya Yamanaka, who showed that the introduction of four specific proteins essential during early embryonic development could be used to convert adult cells into pluripotent cells. Yamanaka was awarded the 2012 Nobel Prize along with Sir John Gurdon for the discovery that mature stem cells can be reprogrammed to become pluripotent.

Production of iPS cells:
• Isolate cells from patient; grow in a dish •
Treat cells with “reprogramming”
• Wait a few weeks
• Pluripotent stem cells
• Change culture conditions to stimulate cells to differentiate into a variety of cell types
• blood cells | gut cells | cardio muscle cells
Credit: Moscow Institute of Physics and Technology
Thanks to their unique regenerative abilities, stem cells offer potential for treating any disease. For example, there have been cases of transplanting retinal pigment epithelium and spine cells from stem cells. Another experiment showed that stem cells were able to regenerate teeth in mice. Reprogramming holds great potential for new medical applications, since reprogrammed pluripotent stem cells (or induced pluripotent stem cells) can be made from a patient’s own cells instead of using pluripotent cells from embryos.
However, the extent of the similarity between induced pluripotent stem cells and human embryonic stem cells remains unclear. Recent studies highlighted significant differences between these two types of stem cells, although only a limited number of cell lines of different origins were analyzed.
Researchers compared induced pluripotent stem cell (iPSC) lines reprogrammed from adult cell types that were previously differentiated from embryonic stem cells. All these cells were isogenic, meaning they all had the same gene set.
Scientists analyzed the transcriptome – the set of all products encoded, synthesized and used in a cell. Moreover, they elicited methylated DNA areas, because methylation plays a critical role in cell specialization. Comprehensive studies of changes in the gene activity regulation mechanism showed similarities between reprogrammed and embryonic stem cells. In addition, researchers produced a list of the activity of 275 key genes that can present reprogramming results.
Researchers studied three types of adult cells – fibroblasts, retinal pigment epithelium and neural cells, all of which consist of the same gene set; but a chemical modification (e.g. methylation) combined with other changes determines which part of DNA will be used for product synthesis.
Scientists concluded that the type of adult cells that were reprogrammed and the process of reprogramming did not leave any marks. Differences between cells that did occur were thought to be the result of random factors.
“We defined the best induced pluripotent stem cells line concept,” says Dmitry Ischenko, MIPT Ph.D. and Institute of Physical Chemical Medicine researcher.
The minimum number of iPSC clones that would be enough for at least one to be similar to embryonic pluripotent cells with 95 percent confidence is five.”
 Clearly, no one is going to convert embryonic stem cells into neurons and reprogram them into induced stem cells. Such a process would be too time-consuming and expensive. This experiment simulated the reprogramming of a patient’s adult cells into induced pluripotent stem cells for further medical use, and even though the reprogramming paper, published in the journal Cell Cycle, does not currently propose a method of organ growth in vitro, it is an important step in the right direction. Both induced pluripotent cells and embryonic stem cells can help researchers understand how specialized cells develop from pluripotent cells. In the future, they may also provide an unlimited supply of replacement cells and tissues that can benefit many patients with diseases that are currently untreatable.
Clearly, no one is going to convert embryonic stem cells into neurons and reprogram them into induced stem cells. Such a process would be too time-consuming and expensive. This experiment simulated the reprogramming of a patient’s adult cells into induced pluripotent stem cells for further medical use, and even though the reprogramming paper, published in the journal Cell Cycle, does not currently propose a method of organ growth in vitro, it is an important step in the right direction. Both induced pluripotent cells and embryonic stem cells can help researchers understand how specialized cells develop from pluripotent cells. In the future, they may also provide an unlimited supply of replacement cells and tissues that can benefit many patients with diseases that are currently untreatable.The study, titled, “An integrative analysis of reprogramming in human isogenic system identified a clone selection criterion,” concluded that reprogramming does not create differences between reprogrammed and embryonic stem cells, involved researchers from the Vavilov Institute of General Genetics, Research Institute of Physical Chemical Medicine, and the Moscow Institute of Physics and Technology (MIPT).
###
- Published in Blog
Stem Cell Research Goes Crimson: International Leader in Stem Cell Research Named New Dean of Harvard Medical School

George Q. Daley, MD, PhD, Harvard Medical School’s newly appointed dean, led dozens of international colleagues in developing ethical guidelines for stem cell research. On March 9, 2009, President Barack H. Obama issued Executive Order 13505: Removing Barriers to Responsible Scientific Research involving Human Stem Cells, stating that the Secretary of Health and Human Services, through the Director of the National Institute of Health (NIH), may support and conduct responsible, scientifically worthy human stem cell research, including human embryonic stem cell (hESC) research, to the extent permitted by law. Internal NIH policies and procedures, consistent with Executive Order 13505 and these Guidelines, govern the conduct of intramural NIH stem cell research.
A prominent stem cell researcher has been named the new dean of Harvard Medical School, the university announced August 9th
George Q. Daley, MD, PhD, who led dozens of international colleagues to unite around ethical guidelines for stem cell research, is taking on a new challenge—unifying the powerful hospitals that train Harvard’s medical students.
taking on a new challenge—unifying the powerful hospitals that train Harvard’s medical students.
Daley will assume the position effective Jan. 1, 2017, succeeding Jeffrey Flier, MD, who stepped down July 31st. Barbara McNeil, MD, the founding head of the Department of Health Care Policy at Harvard Medical School, is filling the position in the interim.
The internationally recognized leader in stem cell science and cancer biology and a longtime member of the Harvard Medical School (HMS) faculty whose work includes the fields of basic science and clinical medicine, Daley was the driving force behind creating international guidelines around first, human embryonic stem cell research, and then the clinical application of stem cells, according to Nancy Witty, CEO of the International Society for Stem Cell Research (ISSCR).
Daley, who cofounded the organization, counseled two dozen scientists through the sensitive ethical discussions involved in establishing stem cell research guidelines, utilized additional input from 60 groups around the world to construct the guidelines which were first published by the National Institute of Health in 2009.
“That’s a very difficult task,” Witty said. “It takes a tremendous amount of diplomacy.” 
Daley is working to adapt insights in stem cell research to improved therapies for genetic and malignant diseases. Important research contributions from his laboratory at Harvard-affiliated Boston Children’s Hospital include the development of customized stem cells to treat genetic immune deficiency in a mouse model (in collaboration with Rudolf Jaenisch, a Professor of Biology at MIT); the differentiation of germ cells from embryonic stem cells (cited as a “Top Ten Breakthrough” by Science magazine in 2003), and the generation of disease-specific pluripotent stem cells by direct reprogramming of human fibroblasts (cited in the “Breakthrough of the Year” issue of Science magazine in 2008).
As a graduate student working with Nobel laureate Dr. David Baltimore, Daley demonstrated that the BCR/ABL oncogene induces chronic myeloid leukemia (CML) in a mouse model, which validated BCR/ABL as a target for drug blockade and encouraged the development of imatinib (GleevecTM; Novartis), a revolutionary magic-bullet chemotherapy that induces remissions in virtually every CML patient. Dr. Daley’s recent studies have clarified mechanisms of Gleevec resistance and informed novel combination chemotherapeutic regimens.
Daley has spent his entire career in Cambridge and Boston, earning a medical degree from Harvard and a PhD in biology from MIT. As Dean of Harvard Med School, Daley’s achievements in stem cell research is expected to shine a distinguished light on the stem cell industry.
Although the position of dean of Harvard Med may be one of the most prominent roles in medicine, the position is not as powerful it might seem: Harvard Med does not directly oversee any hospitals. Instead it relies on 15 affiliated hospitals and clinical sites, which have historically operated as separate, competitive bailiwicks, to train its students and postdoctoral fellows, and support its researchers. Only 151 of the nearly 12,000 people who call themselves Harvard Medical faculty actually work directly for Harvard in its 10 basic science departments.
Daley sees his new position as a congregator who “builds bridges among the institutions” —heavyweight research institutions such as Brigham and Women’s, Massachusetts General, and Boston Children’s hospitals. Persuasiveness, rather than power, is all that Daley says is needed to achieve an alliance.
Daley’s predecessor, Flier, says he spent a full 30 percent to 40 percent of his time as dean trying to build relationships with and coordinate Harvard’s affiliated hospitals and clinics, a challenge Daley says he’s up to. He has a head start in building those relationships through the many positions he has held around Boston’s biomedical community, including chief resident at Mass. General
“My vision is one of increasing connectivity across the community,” Daley says.
Currently a professor of biological chemistry and molecular pharmacology at Harvard Medical School and director of the stem cell transplantation program at Boston Children’s and Dana-Farber Cancer Institute, Daley sees areas of common interest, such as immuno-oncology, which harnesses the body’s own immune system against cancer cells, where the hospitals can work more closely together.
Described by colleagues as a natural leader, Daley recently led an effort to coordinate big-name scientists across several institutions on a collaborative grant to compare two types of stem cells—just one example of how he earned a reputation; he knows how to get different groups talking together in a constructive way.
He also says he wants Harvard Medical’s faculty, students, and staff to reflect the global community the school intends to serve, and that he promotes diversity in hiring for his 30-person lab.
Daley has a keen interest in sickle-cell anemia, which affects people of African descent, including African Americans, and he believes the federal government should invest in a moonshot effort to cure the disease.
Daley plans to continue teaching molecular medicine at Harvard Med after assuming his position as dean. He also plans to spend one day per week in his lab researching blood stem cells.
“It’s important for a dean to remain relevant by continuing to publish papers,” Daley says. “Plus, I just love science.”
Among his priorities is raising money. Despite its worldwide reputation, and its relative influence when it comes to landing federal grants, Harvard Med has seen annual deficits of between $31 million and $45 million for three consecutive years. Suggestions are being made for Harvard to rename its medical school in return for a billion-dollar donation. Daley only says that the idea would be worth considering down the road.
With opportunities for federal grants in decline, Daley says he sees an opportunity to bring in money from corporate partnerships.
For the stem cell research and medical community, Daley’s appointment as dean of Harvard Med is a fitting step toward validating regenerative medicine’s place as an authoritative leader in the future of medicine—one that’s been a long time coming.
Learn more about Dr. Daley here.
###

- Published in Blog
